

Peri-Implantitis: A Clinical Update on Prevalence and Surgical Treatment Outcomes
- PMID: 33800894
- PMCID: PMC7962026
- DOI: 10.3390/jcm10051107
Peri-Implantitis: A Clinical Update on Prevalence and Surgical Treatment Outcomes
Abstract
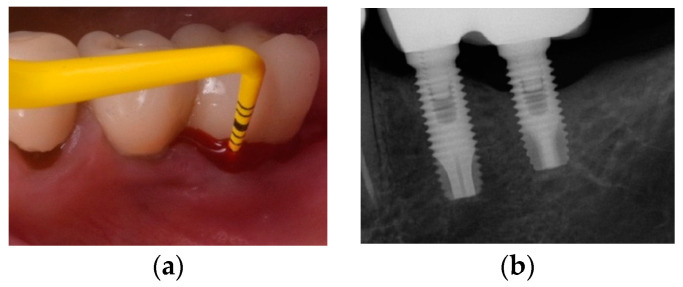
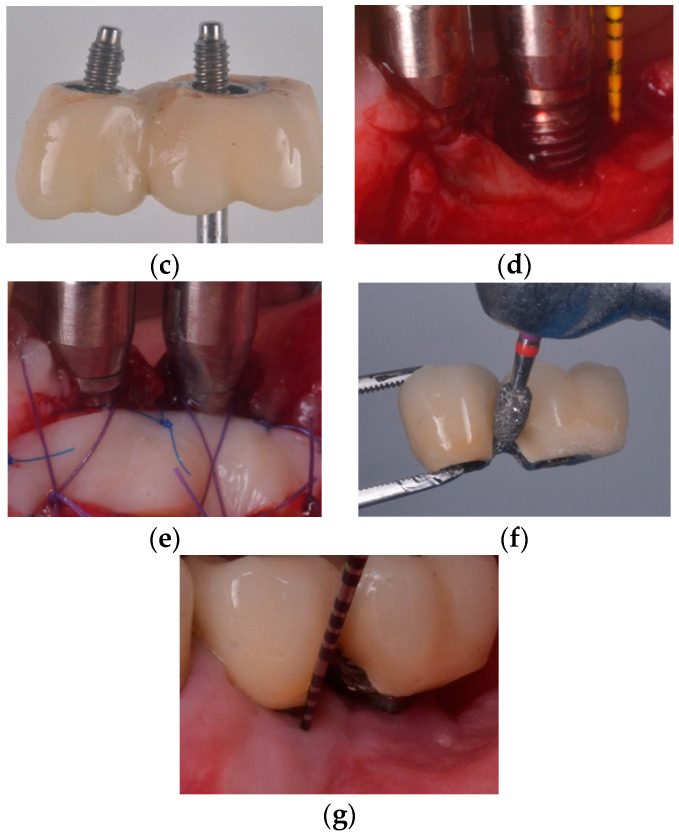
Dental implants may be considered a reliable routine procedure in clinical practice for the replacement of missing teeth. Results from long-term studies indicate that implant-supported dental prostheses constitute a predictable treatment method for the management of fully and partially edentulous patients. Implants and their restorations, however, are not free from biological complications. In fact, peri-implantitis, defined as progressive bone loss associated to clinical inflammation, is not a rare finding nowadays. This constitutes a concern for clinicians and patients given the negative impact on the quality of life and the sequelae originated by peri-implantitis lesions. The purpose of this narrative review is to report on the prevalence of peri-implantitis and to overview the indications, contraindications, complexity, predictability and effectiveness of the different surgical therapeutic modalities to manage this disorder.
Keywords: biological complications; bone regeneration; dental implants; peri-implantitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Berglundh T., Armitage G., Araujo M.G., Gustavo A.-O., Juan B., Paulo M.C., Stephen C., David C., Jan D., Elena F., et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018;89:S313–S318. doi: 10.1002/JPER.17-0739. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
