

High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete
- PMID: 33801229
- PMCID: PMC7957898
- DOI: 10.3390/jcm10050998
High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete
Abstract
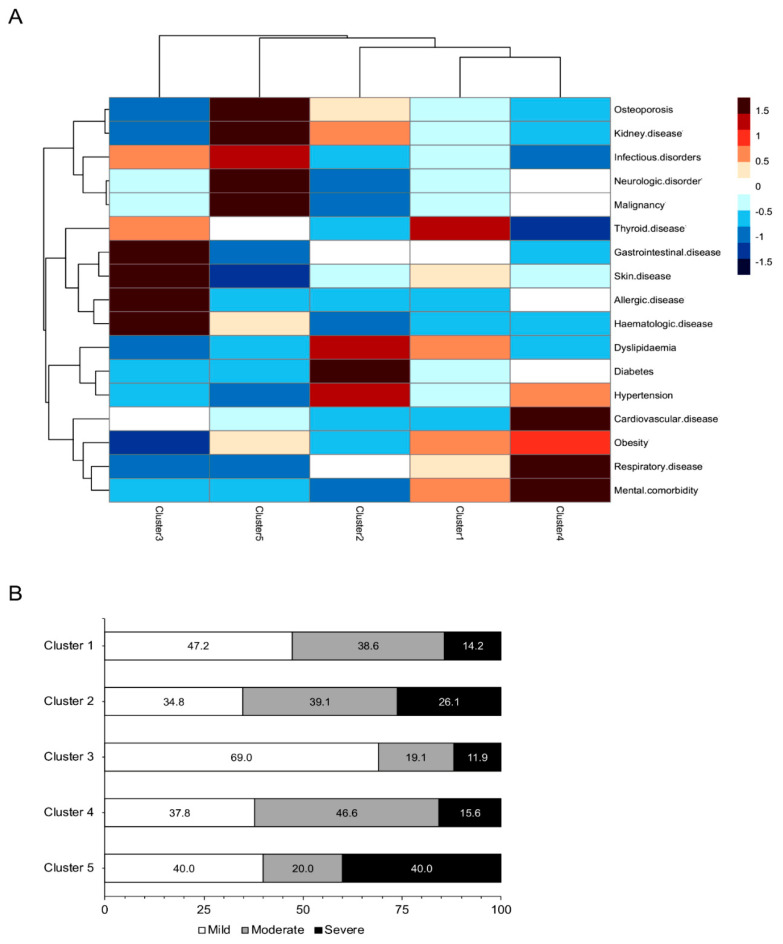
Comorbidities and multimorbidity, often complicating the disease course of patients with chronic inflammatory rheumatic diseases, may be influenced by disease-intrinsic and extrinsic determinants including regional and social factors. We analyzed the frequency and co-segregation of self-reported comorbid diseases in a community-based Mediterranean registry of patients (n = 399) with systemic lupus erythematosus (SLE). Predictors for multimorbidity were identified by multivariable logistic regression, strongly-associated pairs of comorbidities by the Cramer's V-statistic, and comorbidities clusters by hierarchical agglomerative clustering. Among the most prevalent comorbidities were thyroid (45.6%) and metabolic disorders (hypertension: 24.6%, dyslipidemia: 33.3%, obesity: 35.3%), followed by osteoporosis (22.3%), cardiovascular (20.8%), and allergic (20.6%) disorders. Mental comorbidities were also common, particularly depression (26.7%) and generalized anxiety disorder (10.7%). Notably, 51.0% of patients had ≥3 physical and 33.1% had ≥2 mental comorbidities, with a large fraction (n = 86) displaying multimorbidity from both domains. Sociodemographic (education level, marital status) and clinical (disease severity, neurological involvement) were independently associated with physical or mental comorbidity. Patients were grouped into five distinct clusters of variably prevalent comorbid diseases from different organs and domains, which correlated with SLE severity patterns. Conclusively, our results suggest a high multimorbidity burden in patients with SLE at the community, advocating for integrated care to optimize outcomes.
Keywords: autoimmunity; cardiovascular; disease severity; mental disorders; metabolic risk factors; social factors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
The burden of multimorbidity in patients with systemic lupus erythematosus - single-centre analysis.Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2025 Feb 5. doi: 10.5507/bp.2025.004. Online ahead of print. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2025. PMID: 39931935
-
Comorbidities of pediatric systemic lupus erythematosus: A 6-year nationwide population-based study.J Microbiol Immunol Infect. 2016 Apr;49(2):257-63. doi: 10.1016/j.jmii.2014.05.001. Epub 2014 Jul 24. J Microbiol Immunol Infect. 2016. PMID: 25066707
-
Chronic conditions and health problems in rheumatic diseases: comparisons with rheumatoid arthritis, noninflammatory rheumatic disorders, systemic lupus erythematosus, and fibromyalgia.J Rheumatol. 2010 Feb;37(2):305-15. doi: 10.3899/jrheum.090781. Epub 2010 Jan 15. J Rheumatol. 2010. PMID: 20080915
-
The evolving concept of SLE comorbidities.Expert Rev Clin Immunol. 2017 Aug;13(8):753-768. doi: 10.1080/1744666X.2017.1327353. Epub 2017 May 22. Expert Rev Clin Immunol. 2017. PMID: 28471690 Review.
-
The epidemiology of generalized anxiety disorder.Psychiatr Clin North Am. 2001 Mar;24(1):19-39. doi: 10.1016/s0193-953x(05)70204-5. Psychiatr Clin North Am. 2001. PMID: 11225507 Review.
Cited by
-
Exploring the quality of life and comorbidity impact among patients with systemic lupus erythematosus in Saudi Arabia.Saudi Med J. 2024 Oct;45(10):1071-1079. doi: 10.15537/smj.2024.45.10.20240432. Saudi Med J. 2024. PMID: 39379126 Free PMC article.
-
Impact of quality of life on overall work productivity impairment and activity impairment of patients with systemic lupus erythematosus: the PEONY study.Lupus Sci Med. 2025 Jan 19;12(1):e001291. doi: 10.1136/lupus-2024-001291. Lupus Sci Med. 2025. PMID: 39832910 Free PMC article.
-
A Review of Safety Outcomes from Clinical Trials of Baricitinib in Rheumatology, Dermatology and COVID-19.Adv Ther. 2022 Nov;39(11):4910-4960. doi: 10.1007/s12325-022-02281-4. Epub 2022 Sep 5. Adv Ther. 2022. PMID: 36063279 Free PMC article. Review.
-
Integrating electronic health records and GWAS summary statistics to predict the progression of autoimmune diseases from preclinical stages.Nat Commun. 2025 Jan 2;16(1):180. doi: 10.1038/s41467-024-55636-6. Nat Commun. 2025. PMID: 39747168 Free PMC article.
-
High risk of depression, anxiety, and an unfavorable complex comorbidity profile is associated with SLE: a nationwide patient-level study.Arthritis Res Ther. 2022 May 19;24(1):116. doi: 10.1186/s13075-022-02799-6. Arthritis Res Ther. 2022. PMID: 35590393 Free PMC article.
References
-
- Kedves M., Kosa F., Kunovszki P., Takacs P., Szabo M.Z., Karyekar C., Lofland J.H., Nagy G. Large-scale mortality gap between SLE and control population is associated with increased infection-related mortality in lupus. Rheumatology. 2020;59:3443–3451. doi: 10.1093/rheumatology/keaa188. - DOI - PMC - PubMed
-
- Rua-Figueroa I., Lopez-Longo J., Galindo-Izquierdo M., Calvo-Alen J., Del Campo V., Olive-Marques A., Perez-Vicente S., Fernandez-Nebro A., Andres M., Erausquin C., et al. Incidence, associated factors and clinical impact of severe infections in a large, multicentric cohort of patients with systemic lupus erythematosus. Semin. Arthritis Rheum. 2017;47:38–45. doi: 10.1016/j.semarthrit.2017.01.010. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
