

The Need of Enterococcal Coverage in Severe Intra-Abdominal Infection: Evidence from Animal Study
- PMID: 33801494
- PMCID: PMC7958860
- DOI: 10.3390/jcm10051027
The Need of Enterococcal Coverage in Severe Intra-Abdominal Infection: Evidence from Animal Study
Abstract
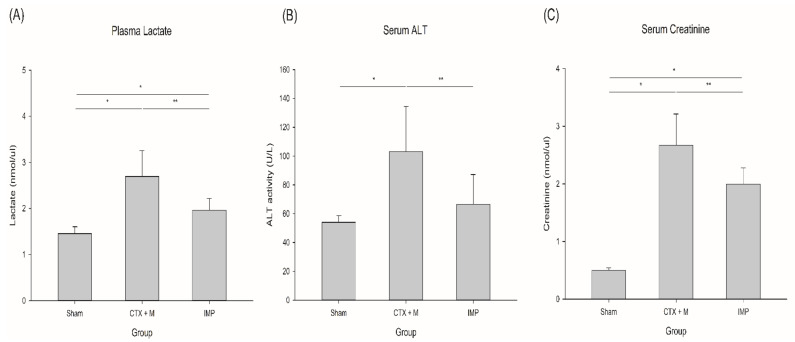
Intra-abdominal infection (IAI) is a common and important cause of infectious mortality in intensive care units. Adequate source control and appropriate antimicrobial regimens are key in the management of IAI. In community-acquired IAI, guidelines recommend the use of different antimicrobial regimens according to severity. However, the evidence for this is weak. We investigated the effect of enterococcal coverage in antimicrobial regimens in a severe polymicrobial IAI model. We investigated the effects of imipenem/cilastatin (IMP) and ceftriaxone with metronidazole (CTX+M) in a rat model of severe IAI. We observed the survival rate and bacterial clearance rate. We identified the bacteria in blood culture. We measured lactate, alanine aminotransferase (ALT), creatinine, interleukin (IL)-6, IL-10, and reactive oxygen species (ROS) in the blood. Endotoxin tolerance of peripheral blood mononuclear cells (PBMCs) was also estimated to determine the level of immune suppression. In the severe IAI model, IMP improved survival and bacterial clearance compared to CTX+M. Enterococcus spp. were more frequently isolated in the CTX+M group. IMP also decreased plasma lactate, cytokine, and ROS levels. ALT and creatinine levels were lower in IMP group. In the mild-to-moderate IAI model, however, there was no survival difference between the groups. Immune suppression of PBMCs was observed in IAI model, and it was more prominent in the severe IAI model. Compared to CTX+M, IMP improved the outcome of rats in severe IAI model.
Keywords: antibiotics; intraabdominal infection; mortality; sepsis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Brun-Buisson C., Doyon F., Carlet J., Dellamonica P., Gouin F., Lepoutre A., Mercier J.C., Offenstadt G., Regnier B. Incidence, risk factors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study in intensive care units. French ICU Group for Severe Sepsis. JAMA. 1995;274:968–974. doi: 10.1001/jama.1995.03530120060042. - DOI - PubMed
-
- DeFrances C.J., Cullen K.A., Kozak L.J. National Hospital Discharge Survey: 2005 annual summary with detailed diagnosis and procedure data. Vital Health Stat. 2007;13:1–209. - PubMed
-
- Solomkin J.S., Mazuski J.E., Bradley J.S., Rodvold K.A., Goldstein E.J., Baron E.J., O’Neill P.J., Chow A.W., Dellinger E.P., Eachempati S.R., et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin. Infect. Dis. 2010;50:133–164. doi: 10.1086/649554. - DOI - PubMed
-
- Mazuski J.E., Tessier J.M., May A.K., Sawyer R.G., Nadler E.P., Rosengart M.R., Chang P.K., O’Neill P.J., Mollen K.P., Huston J.M., et al. The Surgical Infection Society Revised Guidelines on the Management of Intra-Abdominal Infection. Surg. Infect. 2017;18:1–76. doi: 10.1089/sur.2016.261. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
