

Exaggerated Cardiac Contractile Response to Hypoxia in Adults Born Preterm
- PMID: 33802149
- PMCID: PMC7999333
- DOI: 10.3390/jcm10061166
Exaggerated Cardiac Contractile Response to Hypoxia in Adults Born Preterm
Abstract
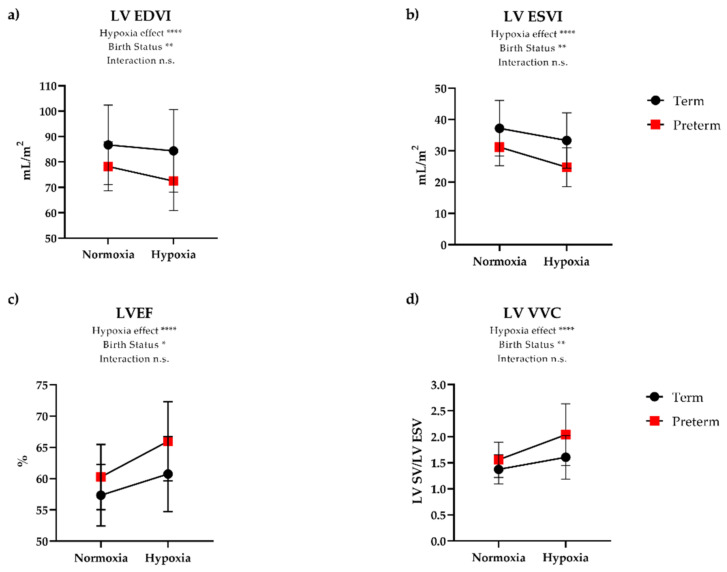
Individuals born prematurely have smaller hearts, cardiac limitations to exercise, and increased overall cardiometabolic risk. The cardiac effects of acute hypoxia exposure as another physiologic stressor remain under explored. The purpose of this study was to determine the effects of hypoxia on ventricular function in adults born preterm. Adults born moderately to extremely preterm (≤32 weeks gestation or <1500 g, N = 32) and born at term (N = 18) underwent cardiac magnetic resonance imaging under normoxic (21% O2) and hypoxic (12% O2) conditions to assess cardiovascular function. In normoxia, cardiac function parameters were similar between groups. During hypoxia, the right ventricular (RV) contractile response was significantly greater in participants born premature, demonstrated by greater increases in RV ejection fraction (EF) (p = 0.002), ventricular-vascular coupling (VVC) (p = 0.004), and strain (p < 0.0001) measures compared to term-born participants, respectively. Left ventricular contractile reserve was similar to term-born participants. Adults born preterm exhibit an exaggerated contractile response to acute hypoxia, particularly in the RV. This suggests that adults born preterm may have contractile reserve, despite the lack of volume reserve identified in previous exercise studies. However, this exaggerated and hyper-adapted response may also increase their risk for late RV failure.
Keywords: cardiac function; contractile response; hypoxia; prematurity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Vogel J.P., Chawanpaiboon S., Watananirun K., Lumbiganon P., Petzold M., Moller A.B., Thinkhamrop J., Laopaiboon M., Seuc A.H., Hogan D., et al. Global, regional and national levels and trends of preterm birth rates for 1990 to 2014: Protocol for development of World Health Organization estimates. Reprod. Health. 2016;13:76. doi: 10.1186/s12978-016-0193-1. - DOI - PMC - PubMed
-
- Goss K.N., Haraldsdottir K., Beshish A.G., Barton G.P., Watson A.M., Palta M., Chesler N.C., Francois C.J., Wieben O., Eldridge M.W. Association Between Preterm Birth and Arrested Cardiac Growth in Adolescents and Young Adults. JAMA Cardiol. 2020;5:910–919. doi: 10.1001/jamacardio.2020.1511. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
