

Efficacy and Safety of Tranexamic Acid in Emergency Trauma: A Systematic Review and Meta-Analysis
- PMID: 33802254
- PMCID: PMC7958951
- DOI: 10.3390/jcm10051030
Efficacy and Safety of Tranexamic Acid in Emergency Trauma: A Systematic Review and Meta-Analysis
Abstract
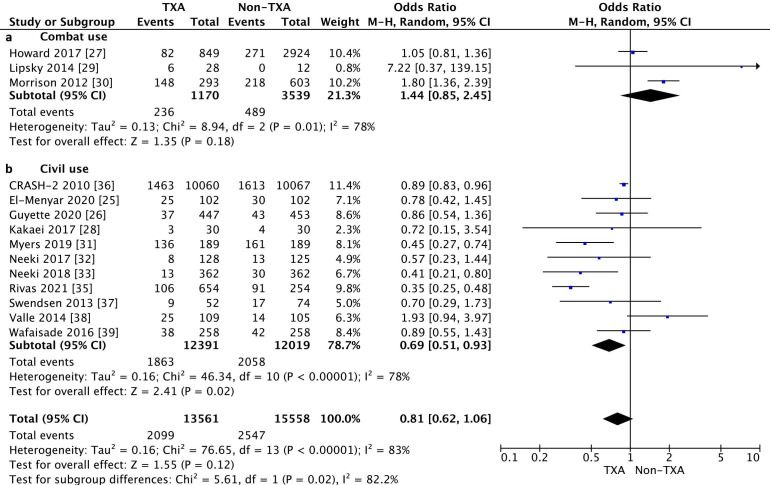
In trauma patients, bleeding can lead to coagulopathy, hemorrhagic shock, and multiorgan failure, and therefore is of fundamental significance in regard to early morbidity. We conducted a meta-analysis to evaluate the efficacy and safety of tranexamic acid (TXA) in civil and military settings and its impact on in-hospital mortality (survival to hospital discharge or 30-day survival), intensive care unit and hospital length of stay, incidence of adverse events (myocardial infarct and neurological complications), and volume of blood product transfusion. The systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A systematic review of the literature using PubMed, Scopus, EMBASE, Web of Science, and the Cochrane Central Register and Controlled Trials (CENTRAL) database was conducted from inception to 10 January 2021. In-hospital mortality was reported in 14 studies and was 15.5% for the TXA group as compared with 16.4% for the non-TXA group (OR = 0.81, 95% CI 0.62-1.06, I2 = 83%, p = 0.12). In a civilian TXA application, in-hospital mortality in the TXA and non-TXA groups amounted to 15.0% and 17.1%, respectively (OR = 0.69, 95% CI 0.51-0.93, p = 0.02, I2 = 78%). A subgroup analysis of the randomized control trial (RCT) studies showed a statistically significant reduction in in-hospital mortality in the TXA group (14.3%) as compared with the non-TXA group (15.7%, OR = 0.89, 95% CI 0.83-0.96, p = 0.003, I2 = 0%). To summarize, TXA used in civilian application reduces in-hospital mortality. Application of TXA is beneficial for severely injured patients who undergoing shock and require massive blood transfusions. Patients who undergo treatment with TXA should be monitored for clinical signs of thromboembolism, since TXA is a standalone risk factor of a thromboembolic event and the D-dimers in traumatic patients are almost always elevated.
Keywords: bleeding; emergency medicine; meta-analysis; mortality; systematic review; tranexamic acid; trauma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Frith D., Goslings J.C., Gaarder C., Maegele M., Cohen M.J., Allard S., Johansson P.I., Stanworth S., Thiemermann C., Brohi K. Definition and drivers of acute traumatic coagulopathy: Clinical and experimental investigations. J. Thromb. Haemost. 2010;8:1919–1925. doi: 10.1111/j.1538-7836.2010.03945.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
