

Non-Incised Papilla Surgical Approach and Leukocyte Platelet-Rich Fibrin in Periodontal Reconstruction of Deep Intrabony Defects: A Case Series
- PMID: 33802261
- PMCID: PMC7967597
- DOI: 10.3390/ijerph18052465
Non-Incised Papilla Surgical Approach and Leukocyte Platelet-Rich Fibrin in Periodontal Reconstruction of Deep Intrabony Defects: A Case Series
Abstract
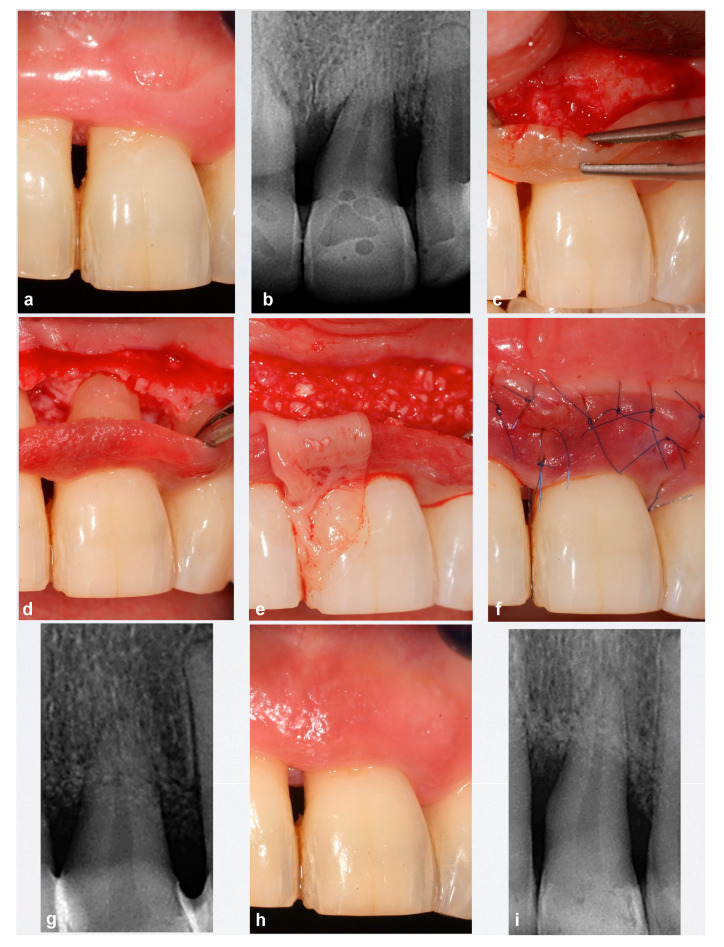
We present the preliminary results of the treatment of teeth with a deep, non-contained periodontal residual defect, vestibular bone dehiscence, and soft tissue recession, by combining an apical non-incised papilla surgical approach (NIPSA) to the defect and leukocyte platelet-rich fibrin (L-PRF) in the vestibular aspect. Four patients (upper left first premolar, upper left central incisor, upper right central incisor and upper right lateral incisor) have been treated. At one year of follow up, all cases showed a considerable reduction in the periodontal pocket depth, a gain in clinical attachment and no bleeding on probing, as well as an improvement in the marginal soft tissue minimizing soft tissue contraction (recession and/or loss of papilla) and improving soft tissue architecture. NIPSA plus L-PRF seem to improve clinical outcomes in deep non-contained intrabony defects associated with soft tissue recession.
Keywords: L-PRF; non-incised papilla surgical approach; periodontitis; reconstructive surgery; regeneration; surgical flaps.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
