

Diagnostic Process Using Endoscopy for Biliary Strictures: A Narrative Review
- PMID: 33802525
- PMCID: PMC7961606
- DOI: 10.3390/jcm10051048
Diagnostic Process Using Endoscopy for Biliary Strictures: A Narrative Review
Abstract
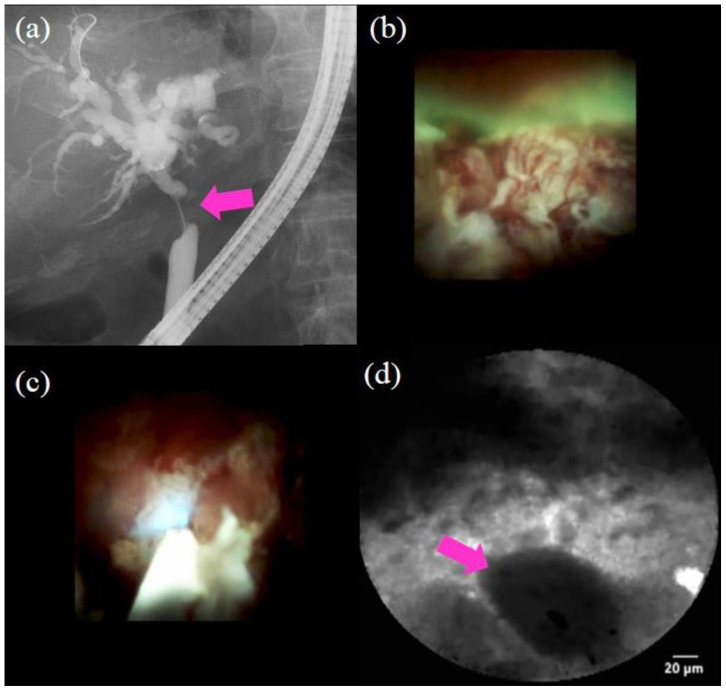
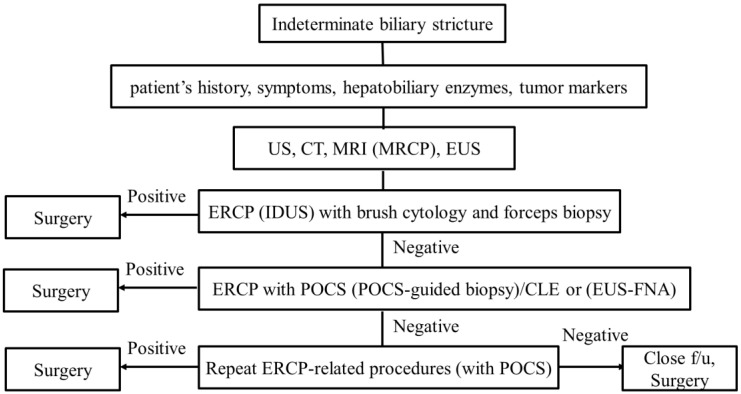
The diagnostic process for biliary strictures remains challenging in some cases. A broad differential diagnosis exists for indeterminate biliary strictures, including benign or malignant lesions. The diagnosis of indeterminate biliary strictures requires a combination of physical examination, laboratory testing, imaging modalities, and endoscopic procedures. Despite the progress of less invasive imaging modalities such as transabdominal ultrasonography, computed tomography, and magnetic resonance imaging, endoscopy plays an essential role in the accurate diagnosis, including the histological diagnosis. Imaging findings and brush cytology and/or forceps biopsy under fluoroscopic guidance with endoscopic retrograde cholangiopancreatography (ERCP) are widely used as the gold standard for the diagnosis of biliary strictures. However, ERCP cannot provide an intraluminal view of the biliary lesion, and its outcomes are not satisfactory. Recently, peroral cholangioscopy, confocal laser endomicroscopy, endoscopic ultrasound (EUS), and EUS-guided fine-needle aspiration have been reported as useful for indeterminate biliary strictures. Appropriate endoscopic modalities need to be selected according to the patient's condition, the lesion, and the expertise of the endoscopist. The aim of this review article is to discuss the diagnostic process for indeterminate biliary strictures using endoscopy.
Keywords: ERCP; EUS; EUS-FNA; biliary strictures; cholangioscopy; confocal laser endomicroscopy; endoscopic retrograde cholangiopancreatography; endoscopic ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Park J., Kim M.H., Kim K.P., Park D.H., Moon S.H., Song T.J., Eum J., Lee S.S., Seo D.W., Lee S.K. Natural History and Prognostic Factors of Advanced Cholangiocarcinoma without Surgery, Chemotherapy, or Radiotherapy: A Large-Scale Observational Study. Gut Liver. 2009;3:298–305. doi: 10.5009/gnl.2009.3.4.298. - DOI - PMC - PubMed
-
- DeOliveira M.L., Cunningham S.C., Cameron J.L., Kamangar F., Winter J.M., Lillemoe K.D., Choti M.A., Yeo C.J., Schulick R.D. Cholangiocarcinoma: Thirty-one-year experience with 564 patients at a single institution. Ann. Surg. 2007;245:755–762. doi: 10.1097/01.sla.0000251366.62632.d3. - DOI - PMC - PubMed
-
- Sano I., Katanuma A., Kuwatani M., Kawakami H., Kato H., Itoi T., Ono M., Irisawa A., Okabe Y., Iwashita T., et al. Long-term outcomes after therapeutic endoscopic retrograde cholangiopancreatography using balloon-assisted enteroscopy for anastomotic stenosis of choledochojejunostomy/pancreaticojejunostomy. J. Gastroenterol. Hepatol. 2019;34:612–619. doi: 10.1111/jgh.14605. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
