

Immune System Alterations in Multiple Myeloma: Molecular Mechanisms and Therapeutic Strategies to Reverse Immunosuppression
- PMID: 33802806
- PMCID: PMC8002455
- DOI: 10.3390/cancers13061353
Immune System Alterations in Multiple Myeloma: Molecular Mechanisms and Therapeutic Strategies to Reverse Immunosuppression
Abstract
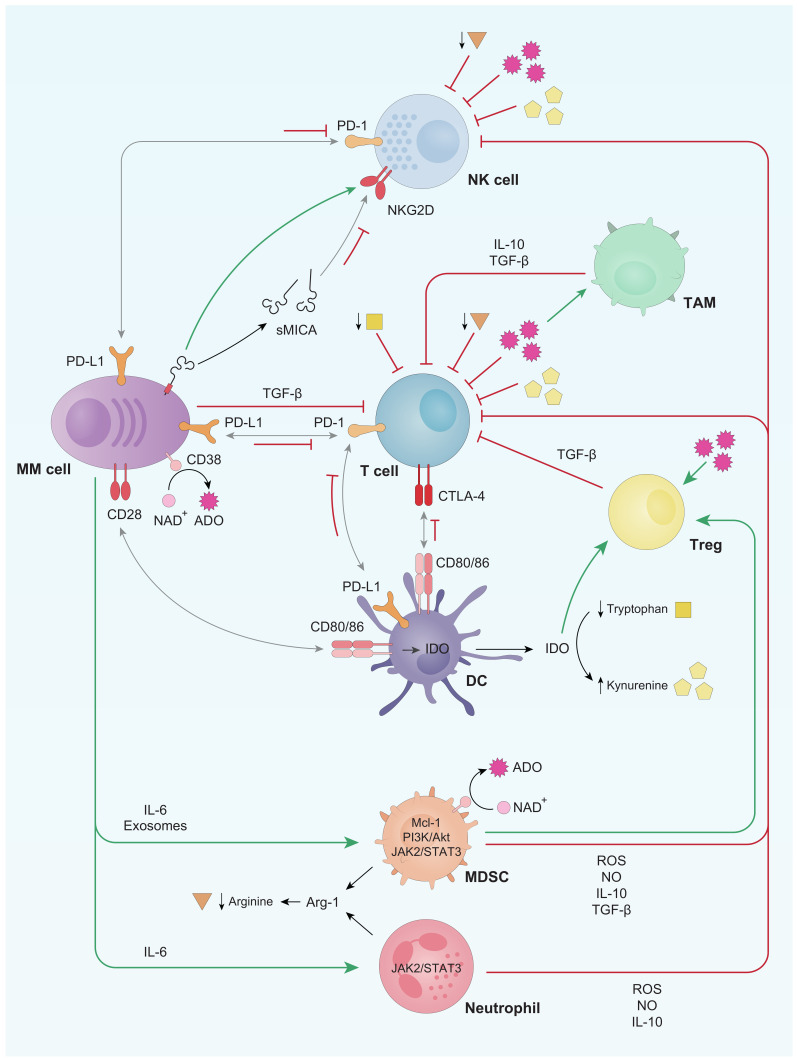
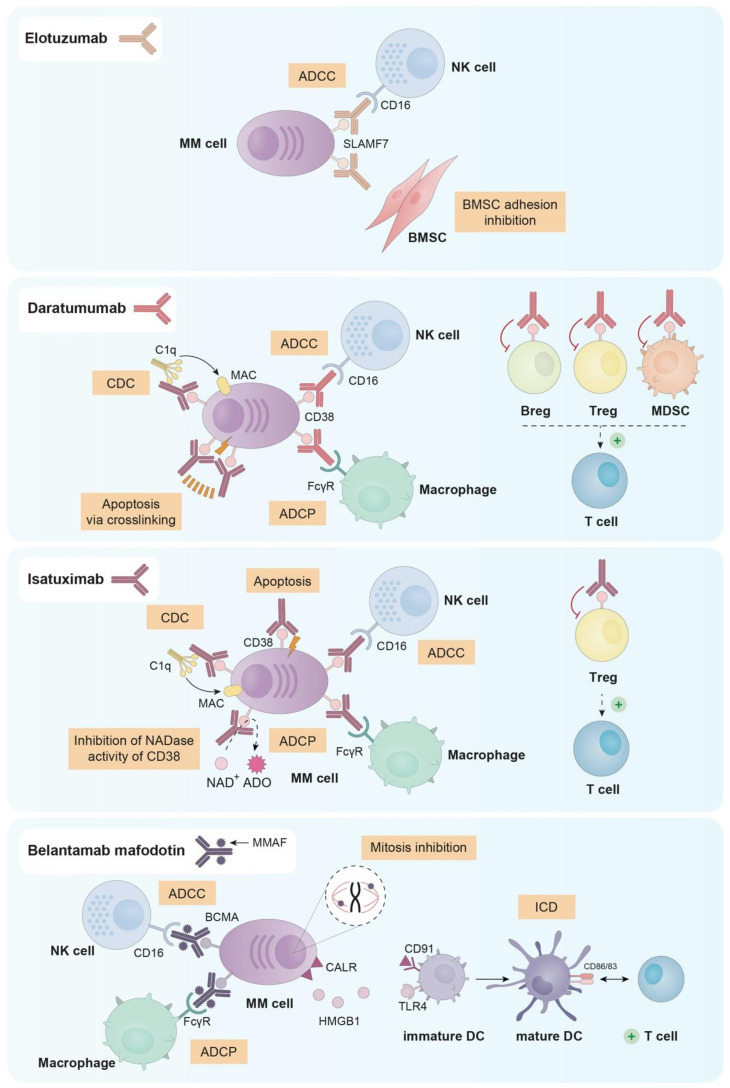
Immunosuppression is a common feature of multiple myeloma (MM) patients and has been associated with disease evolution from its precursor stages. MM cells promote immunosuppressive effects due to both the secretion of soluble factors, which inhibit the function of immune effector cells, and the recruitment of immunosuppressive populations. Alterations in the expression of surface molecules are also responsible for immunosuppression. In this scenario, immunotherapy, as is the case of immunotherapeutic monoclonal antibodies (mAbs), aims to boost the immune system against tumor cells. In fact, mAbs exert part of their cytotoxic effects through different cellular and soluble immune components and, therefore, patients' immunosuppressive status could reduce their efficacy. Here, we will expose the alterations observed in symptomatic MM, as compared to its precursor stages and healthy subjects, in the main immune populations, especially the inhibition of effector cells and the activation of immunosuppressive populations. Additionally, we will revise the mechanisms responsible for all these alterations, including the interplay between MM cells and immune cells and the interactions among immune cells themselves. We will also summarize the main mechanisms of action of the four mAbs approved so far for the treatment of MM. Finally, we will discuss the potential immune-stimulating effects of non-immunotherapeutic drugs, which could enhance the efficacy of immunotherapeutic treatments.
Keywords: immune stimulating drugs; immune system; immunosuppression; monoclonal antibodies; multiple myeloma.
Conflict of interest statement
A.D.-T., M.L.-M., M.G. and T.P. declare no conflict of interest. N.P.: Honoraria: Amgen, Celgene, Janssen, Takeda, The Binding Site; consulting or advisory role: Amgen, Celgene, Janssen, Takeda; speakers’ bureau: Celgene; research funding: Celgene, Janssen, Amgen, Takeda; travel, accommodations, expenses: Amgen, Celgene, Janssen, Takeda. R.G.-S.: Honoraria: Amgen, Astellas, Beigene, BMS, Janssen, Takeda; Speakers bureau/scientific advisory board: Takeda. M.-V.M.: Honoraria: Janssen, Celgene, Amgen, Takeda, GSK, Abbvie, Adaptive, Pfizer, Regeneron, Roche, Gennentech, Oncopeptides, Sanofi.
Figures
References
-
- Rajkumar S.V., Dimopoulos M.A., Palumbo A., Blade J., Merlini G., Mateos M.-V., Kumar S., Hillengass J., Kastritis E., Richardson P., et al. International Myeloma Working Group Updated Criteria for the Diagnosis of Multiple Myeloma. Lancet Oncol. 2014;15:e538–e548. doi: 10.1016/S1470-2045(14)70442-5. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
