

Behavioral and Psychological Symptoms in Dementia (BPSD) and the Use of Antipsychotics
- PMID: 33803277
- PMCID: PMC8002184
- DOI: 10.3390/ph14030246
Behavioral and Psychological Symptoms in Dementia (BPSD) and the Use of Antipsychotics
Abstract
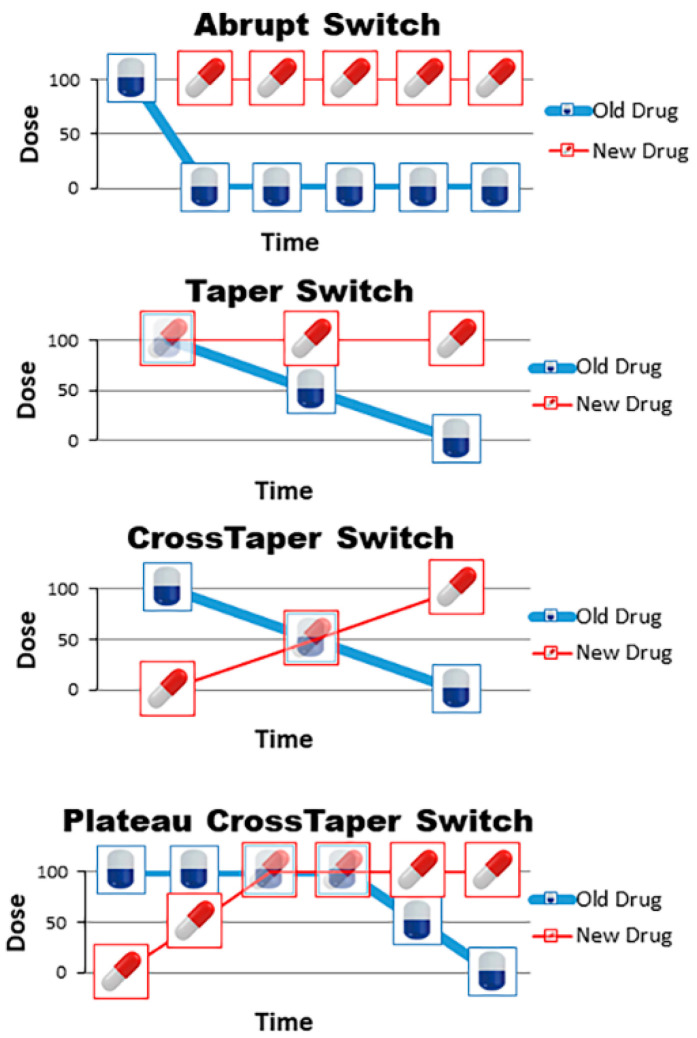
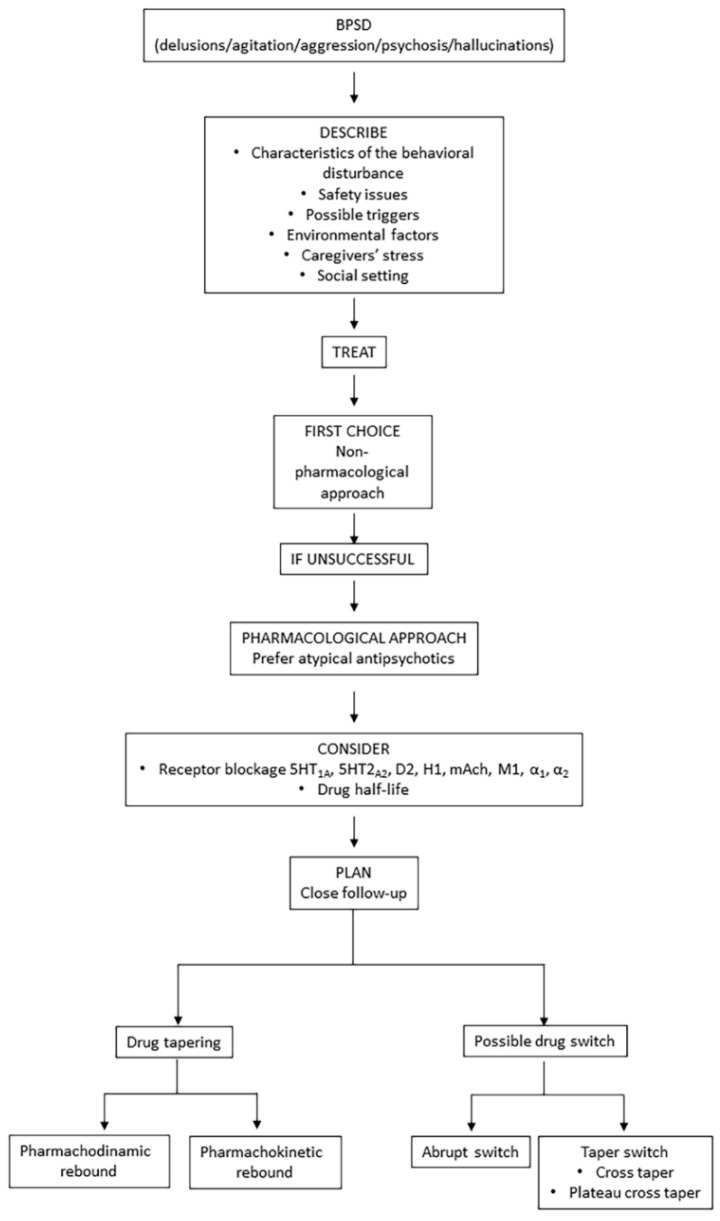
Dementia affects about 47 million people worldwide, number expected to exponentially increase within 30 years. Alzheimer's disease (AD) is the most common dementia type, accounting on its own for almost 70% of all dementia cases. Behavioral and psychological symptoms (BPSD) frequently occur during the disease progression; to treat agitation, aggressiveness, delusions and hallucinations, the use of antipsychotic drugs should be limited, due to their safety issues. In this literature review regarding the use of antipsychotics for treating BPSD in dementia, the advantages and limitation of antipsychotic drugs have been evaluated. The available medications for the management of behavioral and psychological symptoms are the antipsychotics, classed into typical and atypical, depending on their action on dopamine and serotonin receptors. First generation, or typical, antipsychotics exhibit lack of tolerability and display a broad range of side effects such as sedation, anticholinergic effects and extrapyramidal symptoms. Atypical, or second generation, antipsychotics bind more selectively to dopamine receptors and simultaneously block serotonin receptors, resulting in higher tolerability. High attention should be paid to the management of therapy interruption or switch between antipsychotics, to limit the possible rebound effect. Several switching strategies may be adopted, and clinicians should "tailor" therapies, accounting for patients' symptoms, comorbidities, polytherapies and frailty.
Keywords: atypical antipsychotics; behavioral and psychological symptoms of dementia (BPSD); dementia; frailty; typical antipsychotics.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Emmady P.D., Tadi P. Dementia. StatPearls; Treasure Island, FL, USA: 2020.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
