

Thyroid Cancers: From Surgery to Current and Future Systemic Therapies through Their Molecular Identities
- PMID: 33803747
- PMCID: PMC8003273
- DOI: 10.3390/ijms22063117
Thyroid Cancers: From Surgery to Current and Future Systemic Therapies through Their Molecular Identities
Abstract
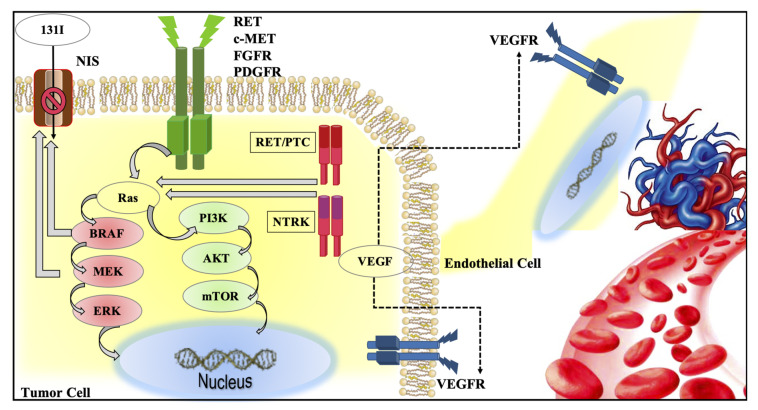
Differentiated thyroid cancers (DTC) are commonly and successfully treated with total thyroidectomy plus/minus radioiodine therapy (RAI). Medullary thyroid cancer (MTC) is only treated with surgery but only intrathyroidal tumors are cured. The worst prognosis is for anaplastic (ATC) and poorly differentiated thyroid cancer (PDTC). Whenever a local or metastatic advanced disease is present, other treatments are required, varying from local to systemic therapies. In the last decade, the efficacy of the targeted therapies and, in particular, tyrosine kinase inhibitors (TKIs) has been demonstrated. They can prolong the disease progression-free survival and represent the most important therapeutic option for the treatment of advanced and progressive thyroid cancer. Currently, lenvatinib and sorafenib are the approved drugs for the treatment of RAI-refractory DTC and PDTC while advanced MTC can be treated with either cabozantinib or vandetanib. Dabrafenib plus trametinib is the only approved treatment by FDA for BRAFV600E mutated ATC. A new generation of TKIs, specifically for single altered oncogenes, is under evaluation in phase 2 and 3 clinical trials. The aim of this review was to provide an overview of the current and future treatments of thyroid cancer with regards to the advanced and progressive cases that require systemic therapies that are becoming more and more targeted on the molecular identity of the tumor.
Keywords: cabozantinib; differentiated thyroid cancer; lenvatinib; medullary thyroid cancer; pralsetinib; selpercatinib; sorafenib; targeted therapy; tyrosine kinase inhibitors; vandetanib.
Conflict of interest statement
R.E. is a consultant for Bayer, EISAI, Loxo, Ipsen, Lilly, Astra Zeneca, Exelixis, Genzyme, but this activity did not influence this work, which has been written independently.
Figures

References
-
- Institute, N.C. Surveillance Epidemiology and End Results Program: SEER Stat Facts: Thyroid Cancer. [(accessed on 16 March 2021)]; Available online: https://seer.cancer.gov/statfacts/html/thyro.html.
-
- Dunlap Q., Davies L. Surgery of the Thyroid and Parathyroid Glands. Elsevier; Amsterdam, The Netherlands: 2021. Differentiated Thyroid Cancer Incidence; pp. 174–180.e2.
-
- Durante C., Haddy N., Baudin E., Leboulleux S., Hartl D., Travagli J.P., Caillou B., Ricard M., Lumbroso J.D., De Vathaire F., et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: Benefits and limits of radioiodine therapy. J. Clin. Endocrinol. Metab. 2006;91:2892–2899. doi: 10.1210/jc.2005-2838. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
