

Against the Resilience of High-Grade Gliomas: The Immunotherapeutic Approach (Part I)
- PMID: 33803885
- PMCID: PMC8003180
- DOI: 10.3390/brainsci11030386
Against the Resilience of High-Grade Gliomas: The Immunotherapeutic Approach (Part I)
Abstract
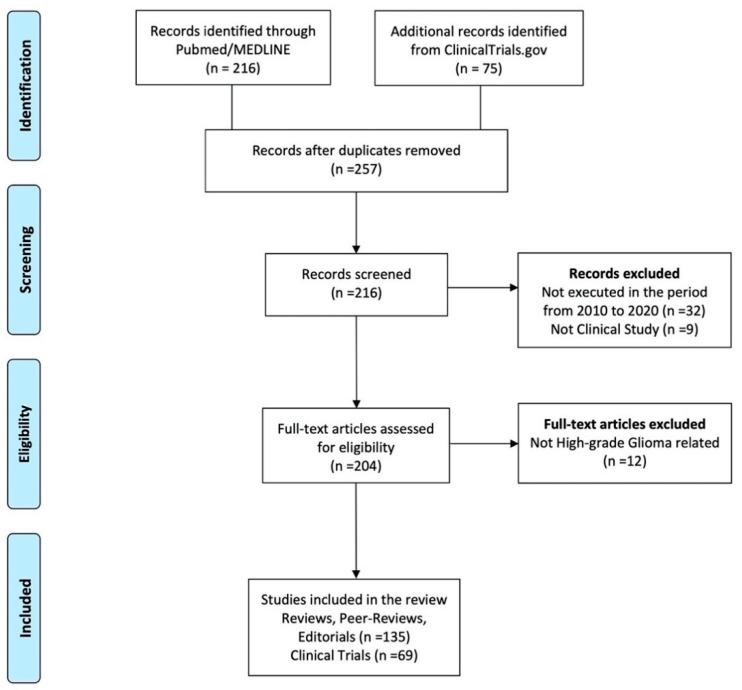
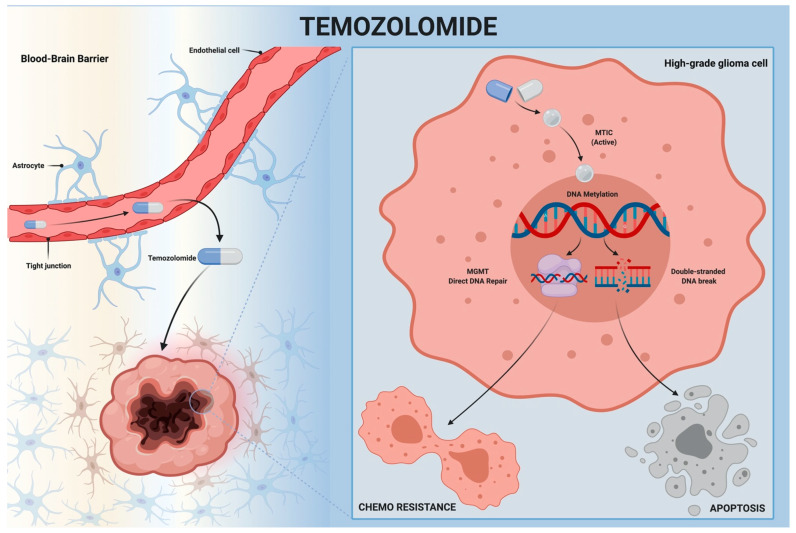
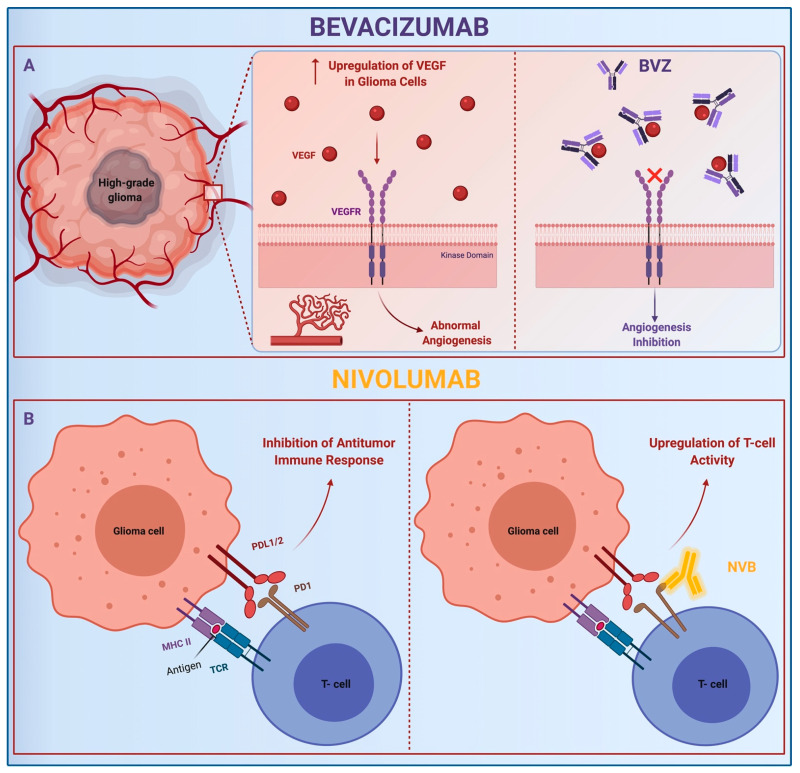
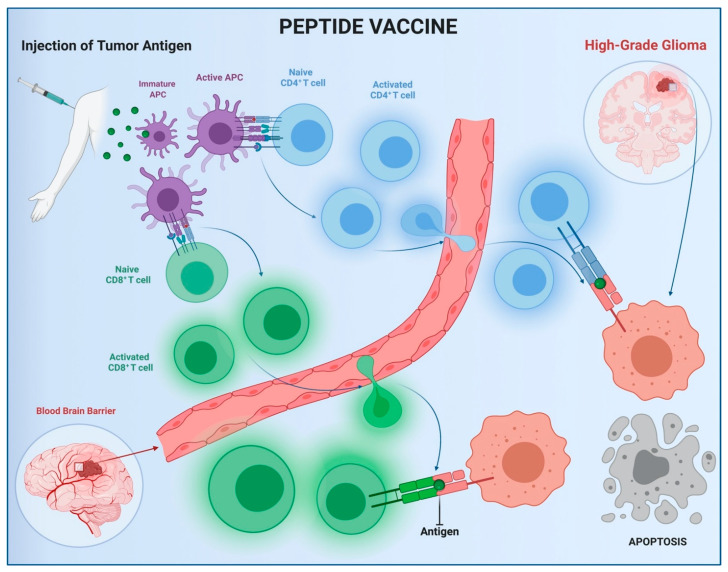
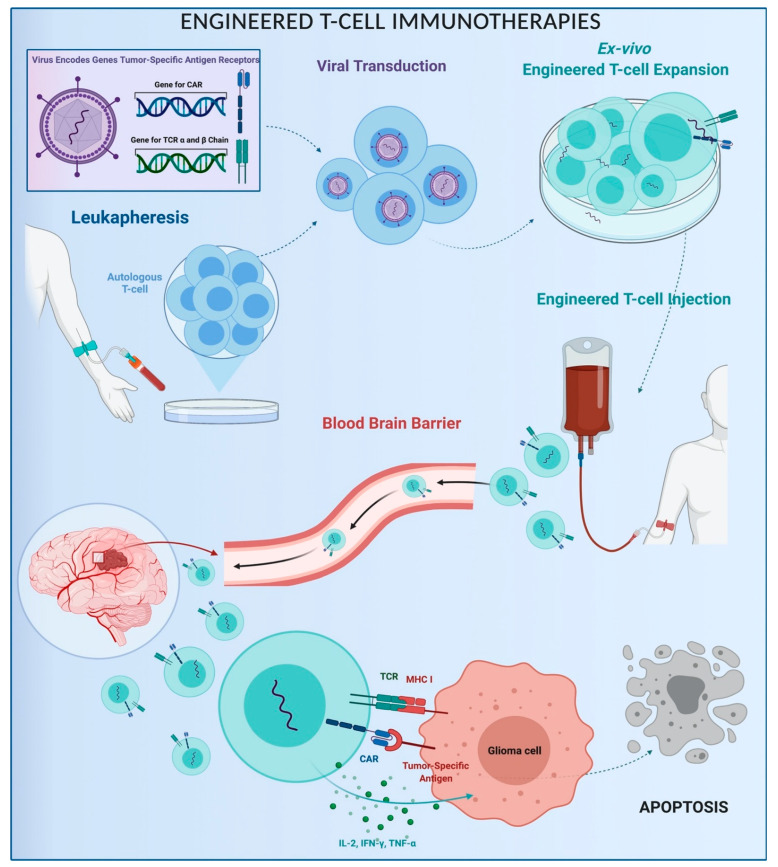
The resilience of high-grade gliomas (HGGs) against conventional chemotherapies is due to their heterogeneous genetic landscape, adaptive phenotypic changes, and immune escape mechanisms. Innovative immunotherapies have been developed to counteract the immunosuppressive capability of gliomas. Nevertheless, further research is needed to assess the efficacy of the immuno-based approach. The aim of this study is to review the newest immunotherapeutic approaches for glioma, focusing on the drug types, mechanisms of action, clinical pieces of evidence, and future challenges. A PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis)-based literature search was performed on PubMed/Medline and ClinicalTrials.gov databases using the keywords "active/adoptive immunotherapy," "monoclonal antibodies," "vaccine," and "engineered T cell.", combined with "malignant brain tumor", "high-grade glioma." Only articles written in English published in the last 10 years were selected, filtered based on best relevance. Active immunotherapies include systemic temozolomide, monoclonal antibodies, and vaccines. In several preclinical and clinical trials, adoptive immunotherapies, including T, natural killer, and natural killer T engineered cells, have been shown to be potential treatment options for relapsing gliomas. Systemic temozolomide is considered the backbone for newly diagnosed HGGs. Bevacizumab and rindopepimut are promising second-line treatments. Adoptive immunotherapies have been proven for relapsing tumors, but further evidence is needed.
Keywords: CAR T cell; bevacizumab; cell-based therapy; glioblastoma; immunotherapy; malignant brain tumor; temozolomide.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ostrom Q.T., Gittleman H., Liao P., Rouse C., Chen Y., Dowling J., Wolinsky Y., Kruchko C., Barnholtz-Sloan J. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2007–2011. Neuro-Oncology. 2014;16:iv1–iv63. doi: 10.1093/neuonc/nou223. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
