

Diabetes during Pregnancy: A Maternal Disease Complicating the Course of Pregnancy with Long-Term Deleterious Effects on the Offspring. A Clinical Review
- PMID: 33803995
- PMCID: PMC7999044
- DOI: 10.3390/ijms22062965
Diabetes during Pregnancy: A Maternal Disease Complicating the Course of Pregnancy with Long-Term Deleterious Effects on the Offspring. A Clinical Review
Abstract
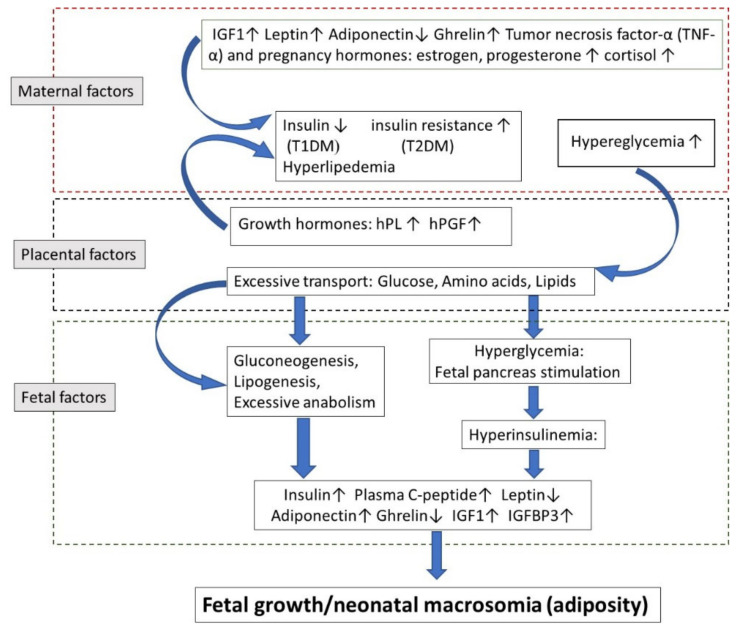
In spite of the huge progress in the treatment of diabetes mellitus, we are still in the situation that both pregestational (PGDM) and gestational diabetes (GDM) impose an additional risk to the embryo, fetus, and course of pregnancy. PGDM may increase the rate of congenital malformations, especially cardiac, nervous system, musculoskeletal system, and limbs. PGDM may interfere with fetal growth, often causing macrosomia, but in the presence of severe maternal complications, especially nephropathy, it may inhibit fetal growth. PGDM may also induce a variety of perinatal complications such as stillbirth and perinatal death, cardiomyopathy, respiratory morbidity, and perinatal asphyxia. GDM that generally develops in the second half of pregnancy induces similar but generally less severe complications. Their severity is higher with earlier onset of GDM and inversely correlated with the degree of glycemic control. Early initiation of GDM might even cause some increase in the rate of congenital malformations. Both PGDM and GDM may cause various motor and behavioral neurodevelopmental problems, including an increased incidence of attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD). Most complications are reduced in incidence and severity with the improvement in diabetic control. Mechanisms of diabetic-induced damage in pregnancy are related to maternal and fetal hyperglycemia, enhanced oxidative stress, epigenetic changes, and other, less defined, pathogenic mechanisms.
Keywords: anomalies; diabetic control; gestational diabetes; growth disturbances; neurodevelopmental problems; perinatal complications; pregestational diabetes; pregnancy.
Conflict of interest statement
None of the authors has any conflict of interest in the preparation of this manuscript.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
