

Novel Histologic Categorization Based on Lauren Histotypes Conveys Prognostic Information for Gastroesophageal Junction Cancers-Analysis from a Large Single Center Cohort in Germany
- PMID: 33804009
- PMCID: PMC8002040
- DOI: 10.3390/cancers13061303
Novel Histologic Categorization Based on Lauren Histotypes Conveys Prognostic Information for Gastroesophageal Junction Cancers-Analysis from a Large Single Center Cohort in Germany
Abstract
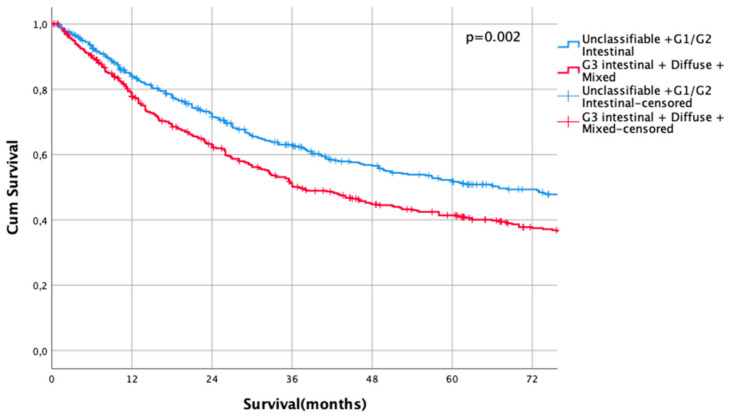
Adenocarcinoma of the gastroesophageal junction (AEG) ranks among the most common cancers in the Western world with increasing incidence. However, the prognostic influence and applicability of the Lauren classification was not examined in detail before. The purpose of this analysis was to analyze the oncologic outcomes of GE-junction cancer related to the Lauren histotype in a large single center cohort. Data from the prospectively documented database of the Klinikum Rechts der Isar (TUM School of Medicine) for patients undergoing curatively intended oncologic resection for GE-junction cancer between 1984 and 2018 were extracted. Univariate and multivariate regression analyses were performed to identify predictors for overall survival. Kaplan-Meier analyses were done to investigate the survival rates according to the Lauren histotype. After identification of two distinct histologic categories with prognostic implications, propensity score matching (PSM) was performed to balance for confounders and evaluate its oncologic outcomes retrospectively. In the time period indicated, 1710 patients were treated for GE-junction cancer. Exclusion criteria were: R2-resections (n = 134), metastatic disease (n = 296), 30-day mortality (n = 45), Siewert type I (n = 21), and missing/incomplete data (n = 61). Finally, 1153 patients were analyzed. In a multiple variable analysis, age, UICC-stage, all Lauren histotypes, R-stage, and postoperative complications were significant predictors of overall survival. Kaplan Meier analysis demonstrated significant survival differences between intestinal, diffuse, and mixed Lauren-histotypes (p = 0.001 and p = 0.029). Survival rates were comparable between non-classifiable and intestinal Lauren-types (p = 0.16) and between diffuse and mixed types (p = 0.56). When combining non-classifiable, well, and moderately differentiated Lauren-types and combining poorly differentiated intestinal, diffuse, and mixed types, two highly prognostic groups were identified (p < 0.0001). This was confirmed after PSM for possible confounders. The Lauren histotypes demonstrate highly prognostic value after oncologic resection of GE-junction cancer (Siewert type II and type III) in a single center Western patient cohort. A simplified histotype classification based on Lauren subtypes revealed a clear distinction of prognostic groups and should be considered for further evaluation.
Keywords: Lauren histotype; gastric/gastroesophageal cancer; perioperative chemotherapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
Significance of Lauren Classification in Patients Undergoing Neoadjuvant/Perioperative Chemotherapy for Locally Advanced Gastric or Gastroesophageal Junction Cancers-Analysis from a Large Single Center Cohort in Germany.Cancers (Basel). 2021 Jan 14;13(2):290. doi: 10.3390/cancers13020290. Cancers (Basel). 2021. PMID: 33466779 Free PMC article.
-
Histopathologic Response Is a Positive Predictor of Overall Survival in Patients Undergoing Neoadjuvant/Perioperative Chemotherapy for Locally Advanced Gastric or Gastroesophageal Junction Cancers-Analysis from a Large Single Center Cohort in Germany.Cancers (Basel). 2020 Aug 11;12(8):2244. doi: 10.3390/cancers12082244. Cancers (Basel). 2020. PMID: 32796715 Free PMC article.
-
UICC Staging after Neoadjuvant/Perioperative Chemotherapy Reveals No Significant Survival Differences Compared to Primary Surgery for Locally Advanced Gastric Cancer.Cancers (Basel). 2022 Dec 14;14(24):6169. doi: 10.3390/cancers14246169. Cancers (Basel). 2022. PMID: 36551654 Free PMC article.
-
Comparison between site N-category and number N-category for nodal staging in carcinoma of the gastroesophageal junction: our experience and literature review.Am Surg. 2006 Feb;72(2):118-23. Am Surg. 2006. PMID: 16536239 Review.
-
Surgical approaches to adenocarcinoma of the gastroesophageal junction: the Siewert II conundrum.Langenbecks Arch Surg. 2017 Dec;402(8):1153-1158. doi: 10.1007/s00423-017-1610-9. Epub 2017 Aug 12. Langenbecks Arch Surg. 2017. PMID: 28803334 Review.
Cited by
-
CT-Derived Quantitative Image Features Predict Neoadjuvant Treatment Response in Adenocarcinoma of the Gastroesophageal Junction with High Accuracy.Cancers (Basel). 2025 Jan 10;17(2):216. doi: 10.3390/cancers17020216. Cancers (Basel). 2025. PMID: 39857998 Free PMC article.
-
Clinicopathological Characteristics and Survival Predictions for Adenocarcinoma of the Esophagogastric Junction: A SEER Population-Based Retrospective Study.Int J Gen Med. 2021 Dec 24;14:10303-10314. doi: 10.2147/IJGM.S341405. eCollection 2021. Int J Gen Med. 2021. PMID: 34992445 Free PMC article.
-
Impact of Clinicopathological Features on Gastric Cancer Stage According to TNM Classification.In Vivo. 2025 Mar-Apr;39(2):1112-1121. doi: 10.21873/invivo.13916. In Vivo. 2025. PMID: 40010943 Free PMC article.
-
Preoperative prediction of the Lauren classification in gastric cancer using automated nnU-Net and radiomics: a multicenter study.Insights Imaging. 2025 Feb 25;16(1):48. doi: 10.1186/s13244-025-01923-9. Insights Imaging. 2025. PMID: 40000513 Free PMC article.
References
-
- Nagtegaal I.D., Odze R.D., Klimstra D., Paradis V., Rugge M., Schirmacher P., Washington M.K., Carneiro F., Cree I.A., The WHO Classification of Tumours Editorial Board The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020;76:182–188. doi: 10.1111/his.13975. - DOI - PMC - PubMed
-
- Mariette C., European Chapter of International Gastric Cancer Association. Carneiro F., Grabsch H.I., Van Der Post R.S., Allum W., De Manzoni G. Consensus on the pathological definition and classification of poorly cohesive gastric carcinoma. Gastric Cancer. 2018;22:1–9. doi: 10.1007/s10120-018-0868-0. - DOI - PubMed
-
- Jiménez Fonseca P., Carmona-Bayonas A., Hernández R., Custodio A., Cano J.M., Lacalle A., Echavarria I., Macias I., Mangas M., Visa L., et al. Lauren subtypes of advanced gastric cancer influence survival and response to chemotherapy: Real-world data from the AGAMENON National Cancer Registry. Br. J. Cancer. 2017;117:775–782. doi: 10.1038/bjc.2017.245. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
