

Severe Acute Kidney Injury in Critically Ill Patients with COVID-19 Admitted to ICU: Incidence, Risk Factors, and Outcomes
- PMID: 33804100
- PMCID: PMC7998509
- DOI: 10.3390/jcm10061217
Severe Acute Kidney Injury in Critically Ill Patients with COVID-19 Admitted to ICU: Incidence, Risk Factors, and Outcomes
Abstract
Background: Critically ill patients with COVID-19 are prone to develop severe acute kidney injury (AKI), defined as KDIGO (Kidney Disease Improving Global Outcomes) stages 2 or 3. However, data are limited in these patients. We aimed to report the incidence, risk factors, and prognostic impact of severe AKI in critically ill patients with COVID-19 admitted to the intensive care unit (ICU) for acute respiratory failure.
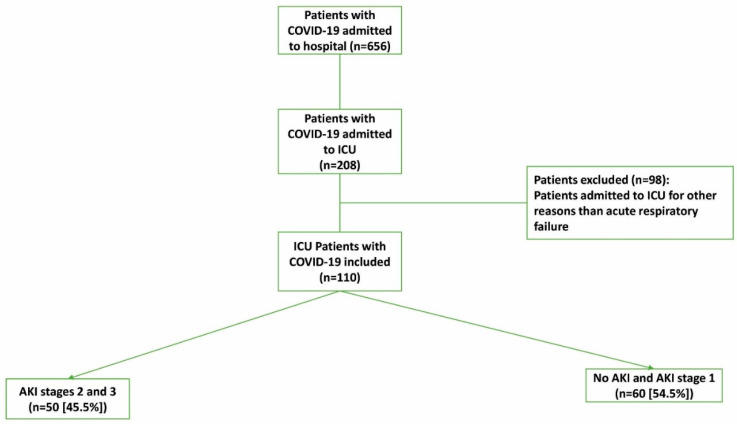
Methods: A retrospective monocenter study including adult patients with laboratory-confirmed severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection admitted to the ICU for acute respiratory failure. The primary outcome was to identify the incidence and risk factors associated with severe AKI (KDIGO stages 2 or 3).
Results: Overall, 110 COVID-19 patients were admitted. Among them, 77 (70%) required invasive mechanical ventilation (IMV), 66 (60%) received vasopressor support, and 9 (8.2%) needed extracorporeal membrane oxygenation (ECMO). Severe AKI occurred in 50 patients (45.4%). In multivariable logistic regression analysis, severe AKI was independently associated with age (odds ratio (OR) = 1.08 (95% CI (confidence interval): 1.03-1.14), p = 0.003), IMV (OR = 33.44 (95% CI: 2.20-507.77), p = 0.011), creatinine level on admission (OR = 1.04 (95% CI: 1.008-1.065), p = 0.012), and ECMO (OR = 11.42 (95% CI: 1.95-66.70), p = 0.007). Inflammatory (interleukin-6, C-reactive protein, and ferritin) or thrombotic (D-dimer and fibrinogen) markers were not associated with severe AKI after adjustment for potential confounders. Severe AKI was independently associated with hospital mortality (OR = 29.73 (95% CI: 4.10-215.77), p = 0.001) and longer hospital length of stay (subhazard ratio = 0.26 (95% CI: 0.14-0.51), p < 0.001). At the time of hospital discharge, 74.1% of patients with severe AKI who were discharged alive from the hospital recovered normal or baseline renal function.
Conclusion: Severe AKI was common in critically ill patients with COVID-19 and was not associated with inflammatory or thrombotic markers. Severe AKI was an independent risk factor of hospital mortality and hospital length of stay, and it should be rapidly recognized during SARS-CoV-2 infection.
Keywords: COVID-19; D-dimer; acute kidney injury; critically ill; intensive care unit; interleukin-6; mechanical ventilation; outcomes.
Conflict of interest statement
The authors declare that they have no competing interests related to the subject of the study. The authors have disclosed that they do not have any potential conflicts of interest.
Figures

References
-
- Yang X., Yu Y., Xu J., Shu H., Xia J., Liu H., Wu Y., Zhang L., Yu Z., Fung M., et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020;8:475–481. doi: 10.1016/S2213-2600(20)30079-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
