

Chronic Diabetic Wounds and Their Treatment with Skin Substitutes
- PMID: 33804192
- PMCID: PMC8001234
- DOI: 10.3390/cells10030655
Chronic Diabetic Wounds and Their Treatment with Skin Substitutes
Abstract
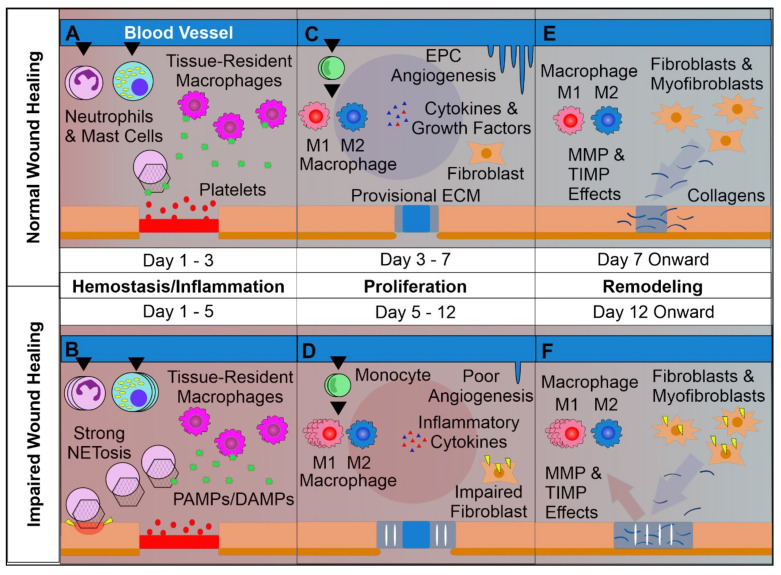
With the global prevalence of type 2 diabetes mellitus steeply rising, instances of chronic, hard-healing, or non-healing diabetic wounds and ulcers are predicted to increase. The growing understanding of healing and regenerative mechanisms has elucidated critical regulators of this process, including key cellular and humoral components. Despite this, the management and successful treatment of diabetic wounds represents a significant therapeutic challenge. To this end, the development of novel therapies and biological dressings has gained increased interest. Here we review key differences between normal and chronic non-healing diabetic wounds, and elaborate on recent advances in wound healing treatments with a particular focus on biological dressings and their effect on key wound healing pathways.
Keywords: chronic wounds; diabetes; matrices; skin dressings; skin substitutes; wound healing.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Cavan D., Fernandez J.D.R., Huang Y., Makaroff L. IDF releases report of global survey on access to medicines and supplies for people with diabetes. Diabetes Res. Clin. Pract. 2017;129:224–225. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
