

Kabuki Syndrome-Clinical Review with Molecular Aspects
- PMID: 33805950
- PMCID: PMC8064399
- DOI: 10.3390/genes12040468
Kabuki Syndrome-Clinical Review with Molecular Aspects
Abstract
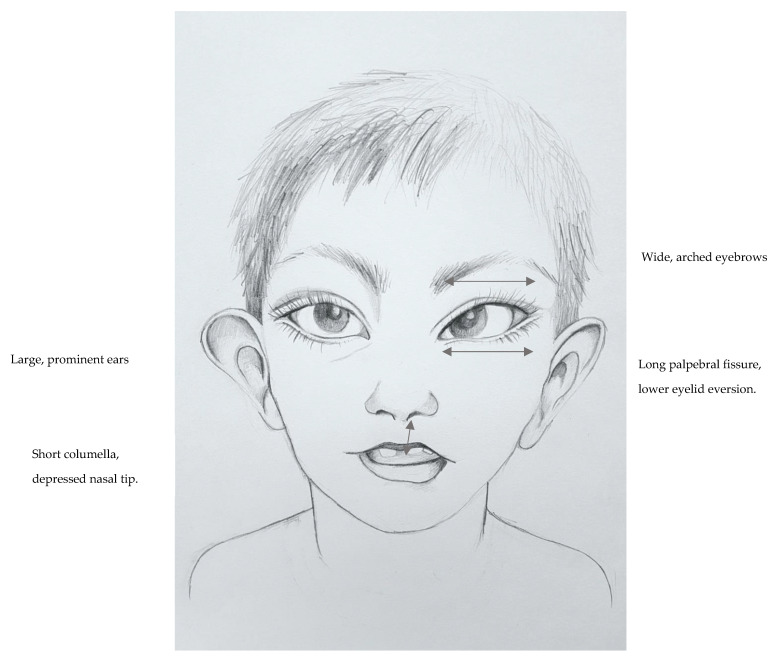
Kabuki syndrome (KS) is a rare developmental disorder principally comprised of developmental delay, hypotonia and a clearly defined dysmorphism: elongation of the structures surrounding the eyes, a shortened and depressed nose, thinning of the upper lip and thickening of the lower lip, large and prominent ears, hypertrichosis and scoliosis. Other characteristics include poor physical growth, cardiac, gastrointestinal and renal anomalies as well as variable behavioral issues, including autistic features. De novo or inherited pathogenic/likely pathogenic variants in the KMT2D gene are the most common cause of KS and account for up to 75% of patients. Variants in KDM6A cause up to 5% of cases (X-linked dominant inheritance), while the etiology of about 20% of cases remains unknown. Current KS diagnostic criteria include hypotonia during infancy, developmental delay and/or intellectual disability, typical dysmorphism and confirmed pathogenic/likely pathogenic variant in KMT2D or KDM6A. Care for KS patients includes the control of physical and psychomotor development during childhood, rehabilitation and multi-specialist care. This paper reviews the current clinical knowledge, provides molecular and scientific links and sheds light on the treatment of Kabuki syndrome individuals.
Keywords: KDM6A; KMT2D; Kabuki syndrome; mechanism; treatment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
