

Pancreatic Cancers with High Grade Tumor Budding Exhibit Hallmarks of Diminished Anti-Tumor Immunity
- PMID: 33806316
- PMCID: PMC7961597
- DOI: 10.3390/cancers13051090
Pancreatic Cancers with High Grade Tumor Budding Exhibit Hallmarks of Diminished Anti-Tumor Immunity
Abstract
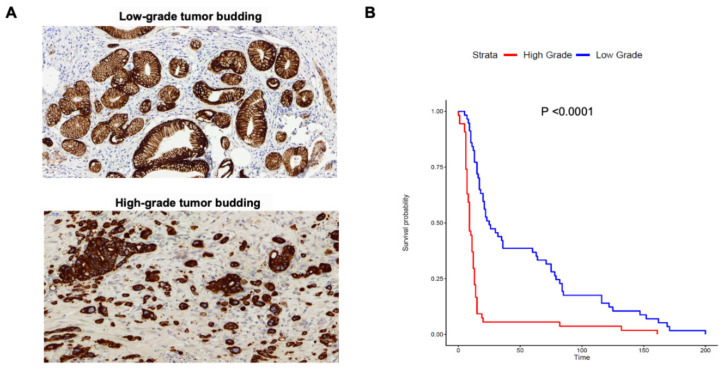
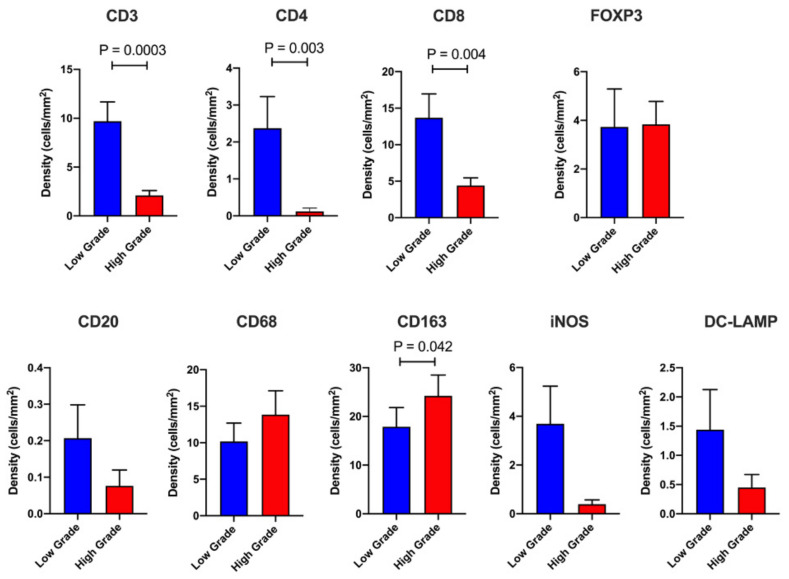
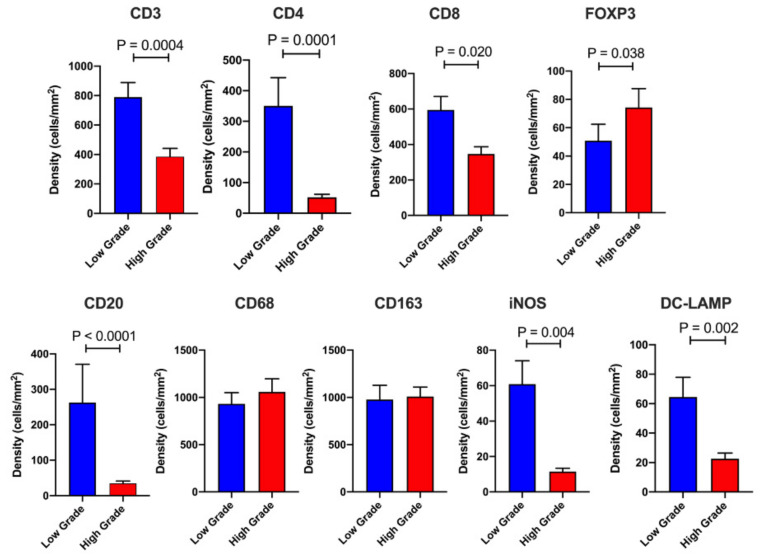
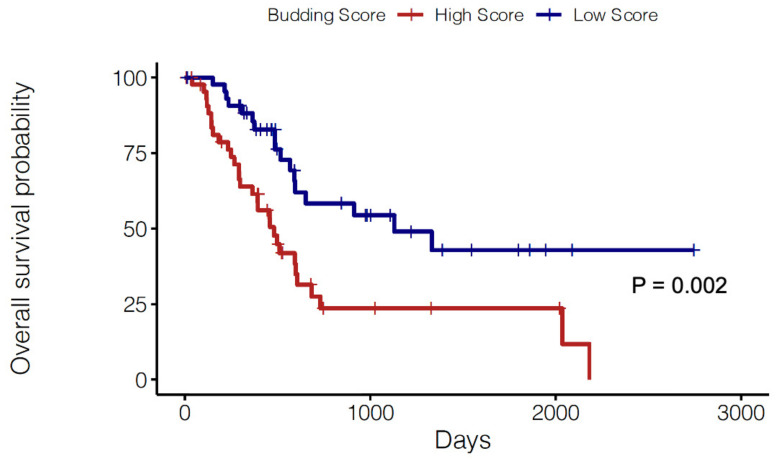
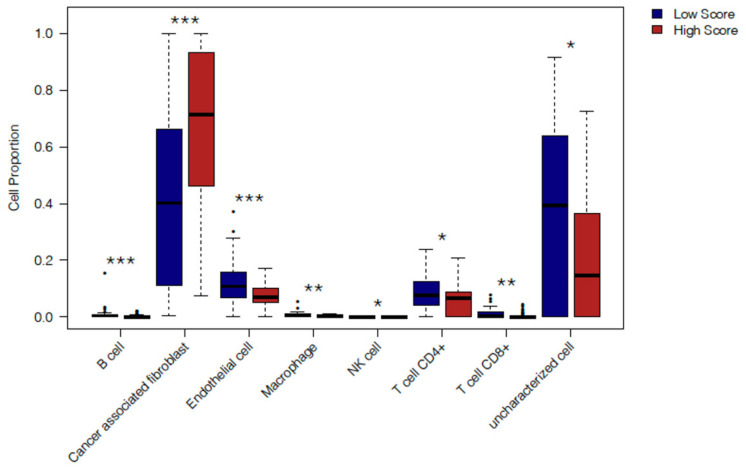
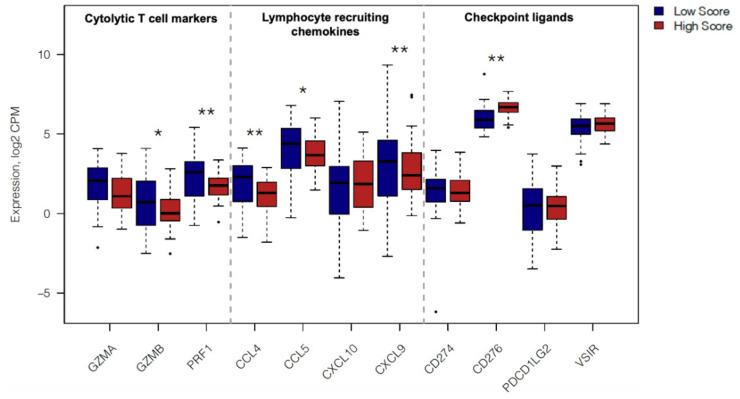
Tumor budding is associated with epithelial-mesenchymal transition and diminished survival in a number of cancer types including pancreatic ductal adenocarcinoma (PDAC). In this study, we dissect the immune landscapes of patients with high grade versus low grade tumor budding to determine the features associated with immune escape and disease progression in pancreatic cancer. We performed immunohistochemistry-based quantification of tumor-infiltrating leukocytes and tumor bud assessment in a cohort of n = 111 PDAC patients in a tissue microarray (TMA) format. Patients were divided based on the ITBCC categories of tumor budding as Low Grade (LG: categories 1 and 2) and High Grade (HG: category 3). Tumor budding numbers and tumor budding grade demonstrated a significant association with diminished overall survival (OS). HG cases exhibit notably reduced densities of stromal (S) and intratumoral (IT) T cells. HG cases also display lower M1 macrophages (S) and increased M2 macrophages (IT). These findings were validated using gene expression data from TCGA. A published tumor budding gene signature demonstrated a significant association with diminished survival in PDAC patients in TCGA. Immune-related gene expression revealed an immunosuppressive TME in PDAC cases with high expression of the budding signature. Our findings highlight a number of immune features that permit an improved understanding of disease progression and EMT in pancreatic cancer.
Keywords: M1/M2 macrophages; T cell-enriched; T lymphocytes; gene signature; pancreatic ductal adenocarcinoma (PDAC); tumor budding.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Raut C.P., Tseng J.F., Sun C.C., Wang H., Wolff R.A., Crane C.H., Hwang R., Vauthey J.-N., Abdalla E.K., Lee J.E., et al. Impact of Resection Status on Pattern of Failure and Survival After Pancreaticoduodenectomy for Pancreatic Adenocarcinoma. Ann. Surg. 2007;246:52–60. doi: 10.1097/01.sla.0000259391.84304.2b. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
