

Existence of a Neutral-Impact Maxillo-Mandibular Displacement on Upper Airways Morphology
- PMID: 33806410
- PMCID: PMC7999116
- DOI: 10.3390/jpm11030177
Existence of a Neutral-Impact Maxillo-Mandibular Displacement on Upper Airways Morphology
Abstract
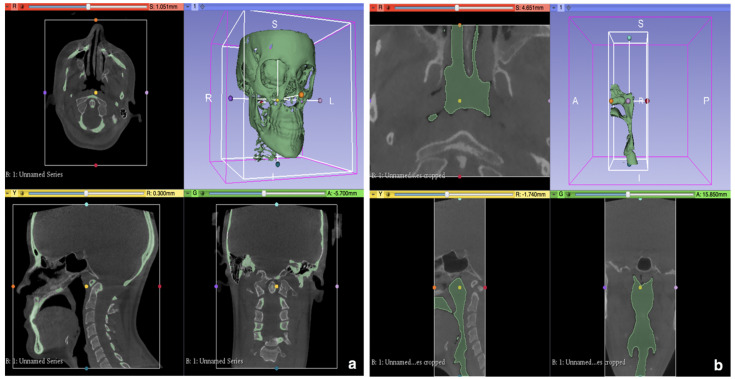
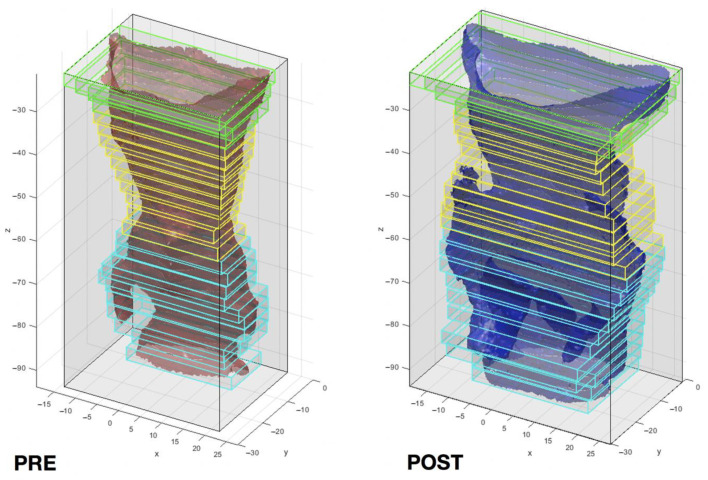
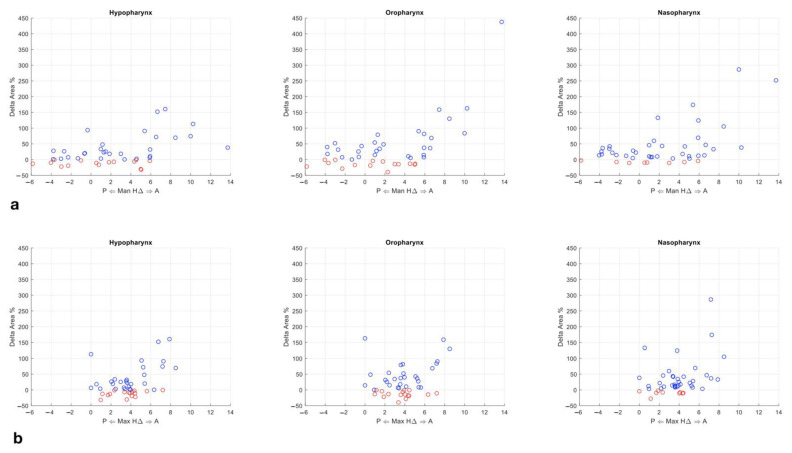
Current scientific evidence on how orthognathic surgery affects the airways morphology remains contradictory. The aim of this study is to investigate the existence and extension of a neutral-impact interval of bony segments displacement on the upper airways morphology. Its upper boundary would behave as a skeletal displacement threshold differentiating minor and major jaw repositioning, with impact on the planning of the individual case. Pre- and post-operative cone beam computed tomographies (CBCTs) of 45 patients who underwent maxillo-mandibular advancement or maxillary advancement/mandibular setback were analysed by means of a semi-automated three-dimensional (3D) method; 3D models of skull and airways were produced, the latter divided into the three pharyngeal subregions. The correlation between skeletal displacement, stacked surface area and volume was investigated. The displacement threshold was identified by setting three ∆Area percentage variations. No significant difference in area and volume emerged from the comparison of the two surgical procedures with bone repositioning below the threshold (approximated to +5 mm). A threshold ranging from +4.8 to +7 mm was identified, varying in relation to the three ∆Area percentages considered. The ∆Area increased linearly above the threshold, while showing no consistency in the interval ranging from -5 mm to +5 mm.
Keywords: 3D analysis method; OSAS; bioengineering; maxillofacial surgery; orthognathic surgery; upper airways.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Bianchi A., Betti E., Tarsitano A., Morselli-Labate A.M., Lancellotti L., Marchetti C. Volumetric three-dimensional computed tomographic evaluation of the upper airway in patients with obstructive sleep apnoea syndrome treated by maxillomandib-ular advancement. Br. J. Oral Maxillofac. Surg. 2014;52:831–837. doi: 10.1016/j.bjoms.2014.07.101. - DOI - PubMed
-
- Yamashita A.L., Filho L.I., Leite P.C.C., Navarro R.D.L., Ramos A.L., Previdelli I.T.S., Ribeiro M.H.D.M., Iwaki L.C.V. Three-dimensional analysis of the pharyngeal airway space and hyoid bone position after orthognathic surgery. J. Cranio-Maxillofacial Surg. 2017;45:1408–1414. doi: 10.1016/j.jcms.2017.06.016. - DOI - PubMed
-
- Swennen R.J. 3D Virtual Treatment Planning of Orthognathic Surgery. Springer; Berlin/Heidelberg, Germany: 2017. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
