

Low Sensitivity of Admission Lung US Compared to Chest CT for Diagnosis of Lung Involvement in a Cohort of 82 Patients with COVID-19 Pneumonia
- PMID: 33806432
- PMCID: PMC8001137
- DOI: 10.3390/medicina57030236
Low Sensitivity of Admission Lung US Compared to Chest CT for Diagnosis of Lung Involvement in a Cohort of 82 Patients with COVID-19 Pneumonia
Abstract
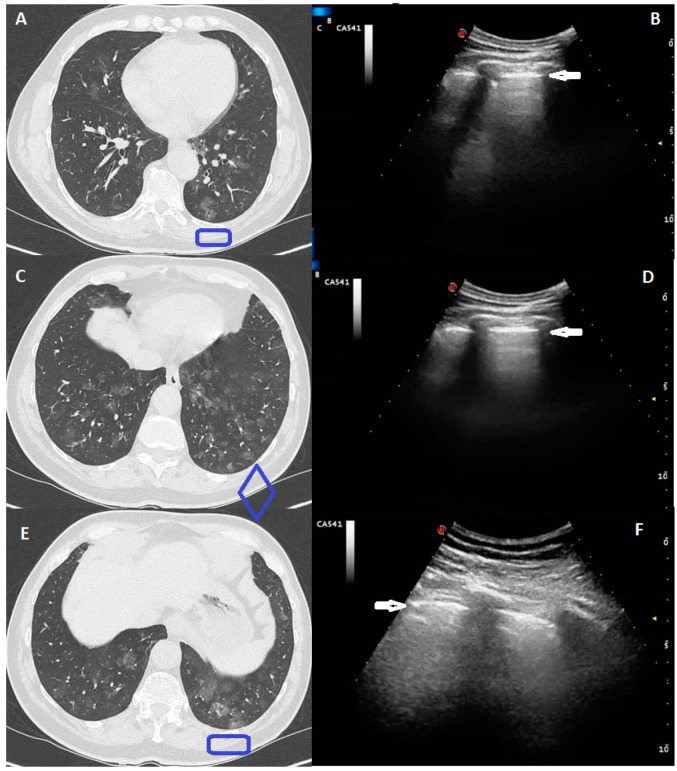
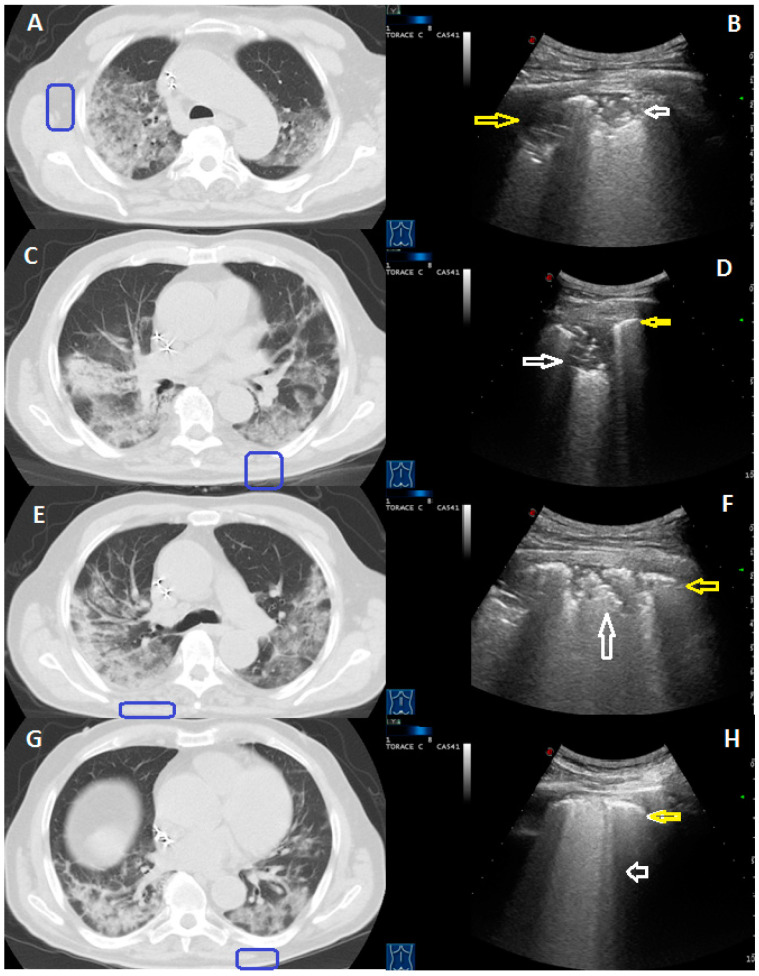
Background and Objectives: The potential role of lung ultrasound (LUS) in characterizing lung involvement in Coronavirus disease 2019 (COVID-19) is still debated. The aim of the study was to estimate sensitivity of admission LUS for the detection of SARS-CoV-2 lung involvement using Chest-CT (Computed Tomography) as reference standard in order to assess LUS usefulness in ruling out COVID-19 pneumonia in the Emergency Department (ED). Methods: Eighty-two patients with confirmed COVID-19 and signs of lung involvement on Chest-CT were consecutively admitted to our hospital and recruited in the study. Chest-CT and LUS examination were concurrently performed within the first 6-12h from admission. Sensitivity of LUS was calculated using CT findings as a reference standard. Results: Global LUS sensitivity in detecting COVID-19 pulmonary lesions was 52%. LUS sensitivity ranged from 8% in case of focal and sporadic ground-glass opacities (mild disease), to 52% for a crazy-paving pattern (moderate disease) and up to 100% in case of extensive subpleural consolidations (severe disease), although LUS was not always able to detect all the consolidations assessed at Chest-CT. LUS sensitivity was higher in detecting a typical Chest-CT pattern (60%) and abnormalities showing a middle-lower zone predominance (79%). Conclusions: As admission LUS may result falsely negative in most cases, it should not be considered as a reliable imaging tool in ruling out COVID-19 pneumonia in patients presenting in ED. It may at least represent an expanded clinical evaluation that needs integration with other diagnostic tests (e.g., nasopharyngeal swab, Chest-CT).
Keywords: COVID-19; Chest-CT; SARS-CoV-2 pneumonia; interstitial pneumonia; lung ultrasound (LUS); sensitivity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- WHO Pneumonia of Unknown Cause–China. [(accessed on 30 May 2020)];2020 Available online: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-ch...
-
- WHO Announces-COVID-19 Outbreak a Pandemic. [(accessed on 30 May 2020)];2020 Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus....
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
