

Real-World Clinical Management of Patients with Primary Biliary Cholangitis-A Retrospective Multicenter Study from Germany
- PMID: 33806503
- PMCID: PMC7961881
- DOI: 10.3390/jcm10051061
Real-World Clinical Management of Patients with Primary Biliary Cholangitis-A Retrospective Multicenter Study from Germany
Abstract
Background: Clinical practice guidelines for patients with primary biliary cholangitis (PBC) have been recently revised and implemented for well-established response criteria to standard first-line ursodeoxycholic acid (UDCA) therapy at 12 months after treatment initiation for the early identification of high-risk patients with inadequate treatment responses who may require treatment modification. However, there are only very limited data concerning the real-world clinical management of patients with PBC in Germany.
Objective: The aim of this retrospective multicenter study was to evaluate response rates to standard first-line UDCA therapy and subsequent Second-line treatment regimens in a large cohort of well-characterized patients with PBC from 10 independent hepatological referral centers in Germany prior to the introduction of obeticholic acid as a licensed second-line treatment option.
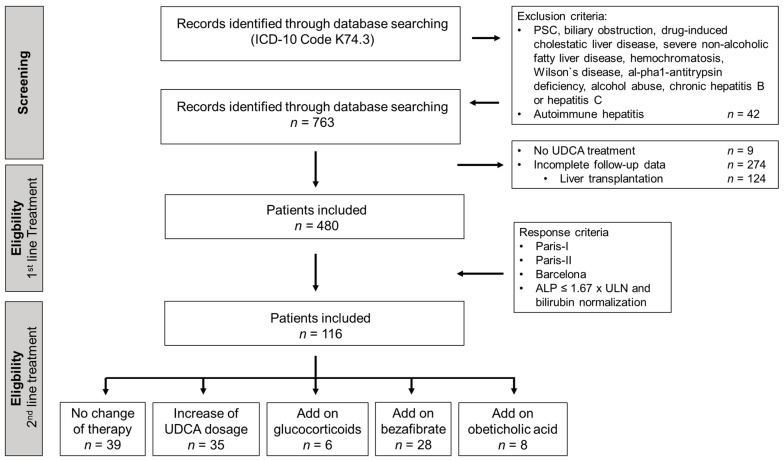
Methods: Diagnostic confirmation of PBC, standard first-line UDCA treatment regimens and response rates at 12 months according to Paris-I, Paris-II, and Barcelona criteria, the follow-up cut-off alkaline phosphatase (ALP) ≤ 1.67 × upper limit of normal (ULN) and the normalization of bilirubin (bilirubin ≤ 1 × ULN) were retrospectively examined between June 1986 and March 2017. The management and hitherto applied second-line treatment regimens in patients with an inadequate response to UDCA and subsequent response rates at 12 months were also evaluated.
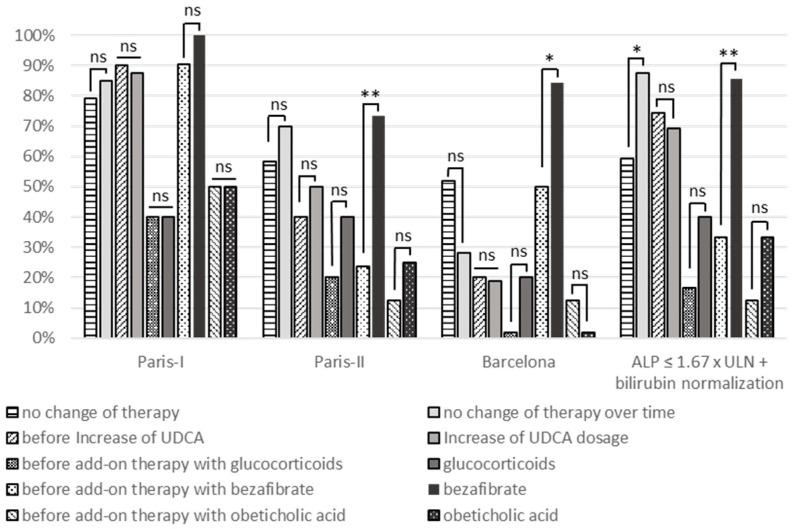
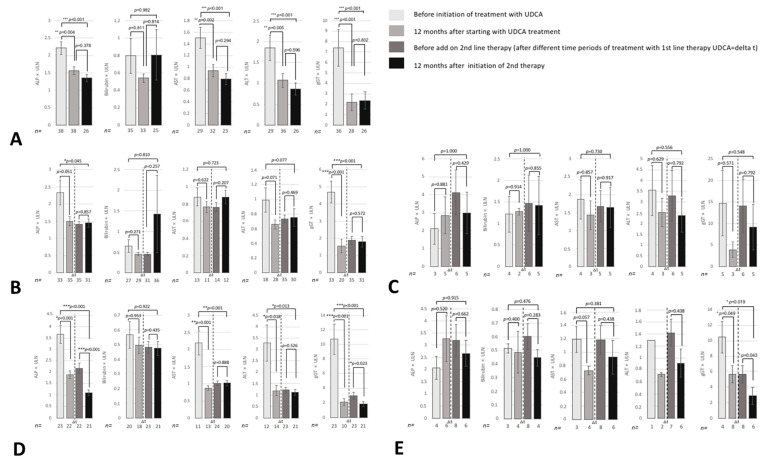
Results: Overall, 480 PBC patients were included in this study. The median UDCA dosage was 13.2 mg UDCA/kg bodyweight (BW)/d. Adequate UDCA treatment response rates according to Paris-I, Paris-II, and Barcelona criteria were observed in 91, 71.3, and 61.3% of patients, respectively. In 83.8% of patients, ALP ≤ 1.67 × ULN were achieved. A total of 116 patients (24.2%) showed an inadequate response to UDCA according to at least one criterion. The diverse second-line treatment regimens applied led to significantly higher response rates according to Paris-II (35 vs. 60%, p = 0.005), Barcelona (13 vs. 34%, p = 0.0005), ALP ≤ 1.67 × ULN and bilirubin ≤ 1 × ULN (52.1 vs. 75%, p = 0.002). The addition of bezafibrates appeared to induce the strongest beneficial effect in this cohort (Paris II: 24 vs. 74%, p = 0.004; Barcelona: 50 vs. 84%, p = 0.046; ALP < 1.67 × ULN and bilirubin ≤ 1 × ULN: 33 vs. 86%, p = 0.001).
Conclusion: Our large retrospective multicenter study confirms high response rates following UDCA first-line standard treatment in patients with PBC and highlights the need for close monitoring and early treatment modification in high-risk patients with an insufficient response to UDCA since early treatment modification significantly increases subsequent response rates of these patients.
Keywords: autoantibodies; primary biliary cholangitis; second line therapy; treatment response; ursodeoxycholic acid.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Lammert C., Juran B.D., Schlicht E., Chan L.L., Atkinson E.J., de Andrade M., Lazaridis K.N. Biochemical response to ursodeoxycholic acid predicts survival in a North American cohort of primary biliary cirrhosis patients. J. Gastroenterol. 2014;49:1414–1420. doi: 10.1007/s00535-013-0903-1. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
