

Sport and Dental Traumatology: Surgical Solutions and Prevention
- PMID: 33806915
- PMCID: PMC8005016
- DOI: 10.3390/dj9030033
Sport and Dental Traumatology: Surgical Solutions and Prevention
Abstract
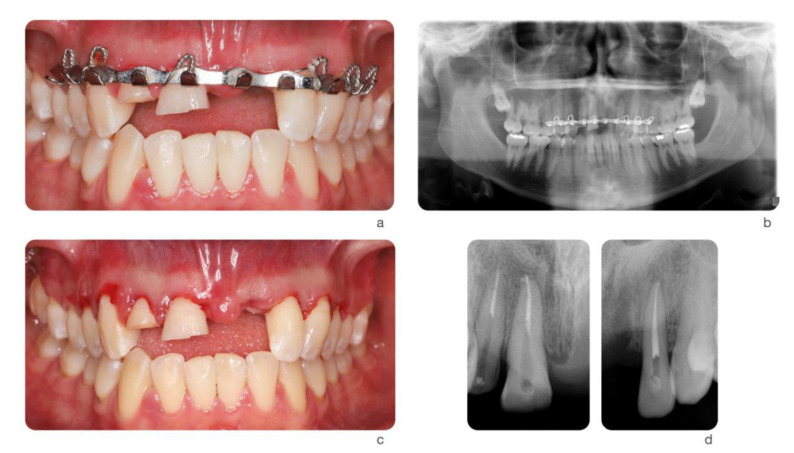
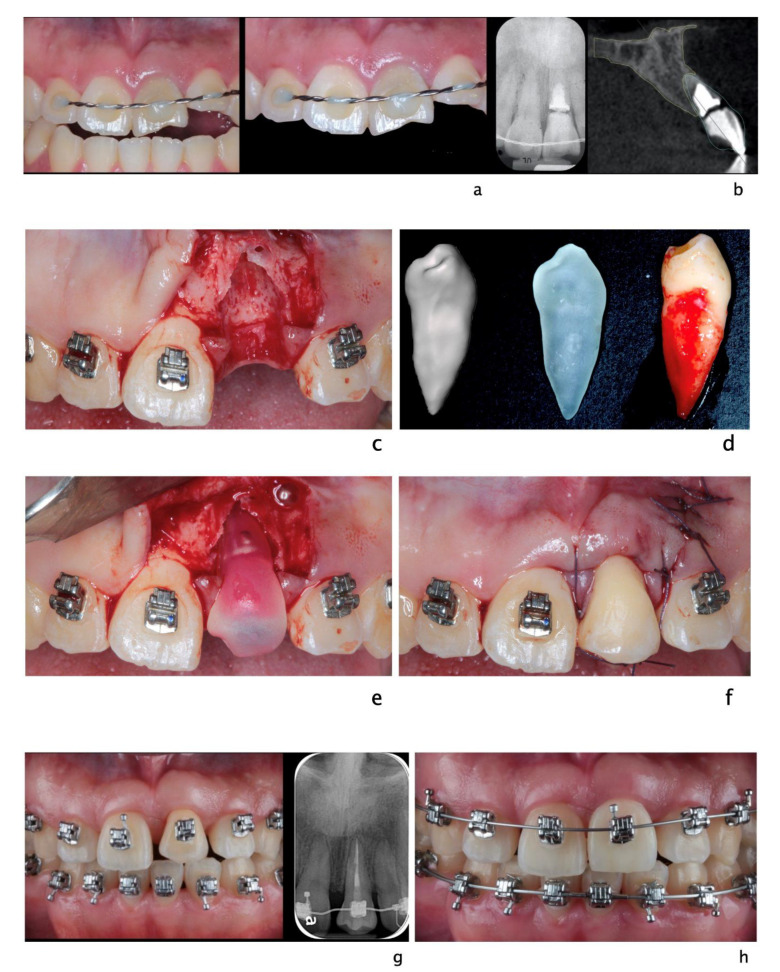
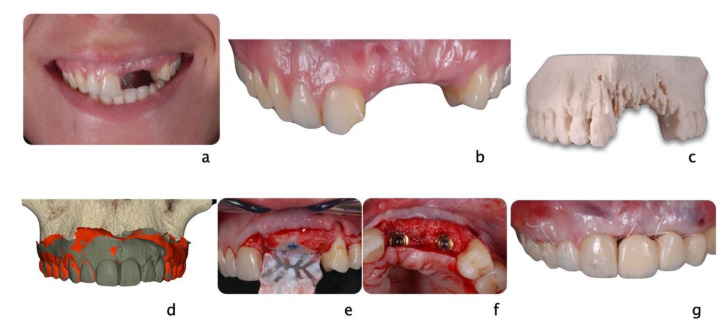
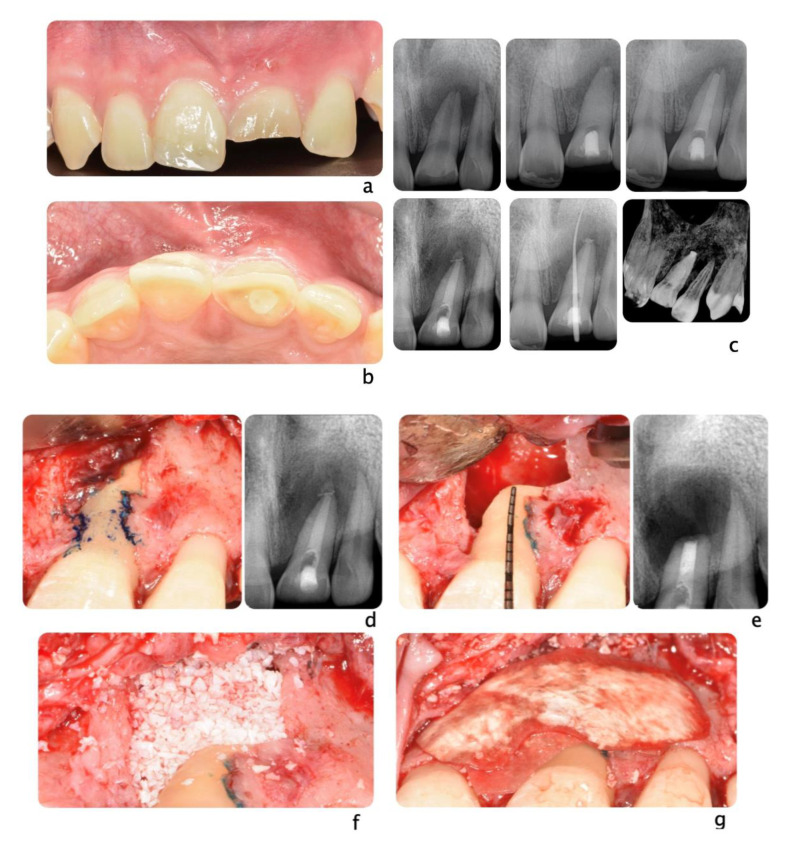
Trauma is a worldwide cause of millions of deaths and severe injuries every year, all over the world. Despite the limited extension of the oral region compared to the whole body, dental and oral injuries account for a fairly high percentage of all body traumas. Among head and neck traumas, dental and facial injuries are highly correlated to sport activities, and their management can be a real challenge for practitioners of any specialty. In case of trauma directed to periodontal structures, restorative and endodontic solutions may not be sufficient to achieve a definitive and long-lasting treatment. This article aims to illustrate surgical options and appliances to prevent dental injuries that may be available to the clinicians treating dental trauma involving oral soft and hard tissues.
Keywords: dental implants; dental trauma; facial injury; periodontology; tooth auto-transplantation.
Conflict of interest statement
Authors report no conflict of interest.
Figures


References
-
- World Health Organization . Injuries and Violence: The Facts 2014. World Health Organization; Geneva, Switzerland: 2014.
-
- Petersson E.E., Andersson L., Sörensen S. Traumatic Oral Vs Non-Oral Injuries. Swed. Dent. J. 1997;21:55–68. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
