

Immune Checkpoints Inhibitors and Chemotherapy as First-Line Treatment for Metastatic Urothelial Carcinoma: A Network Meta-Analysis of Randomized Phase III Clinical Trials
- PMID: 33807108
- PMCID: PMC8005008
- DOI: 10.3390/cancers13061484
Immune Checkpoints Inhibitors and Chemotherapy as First-Line Treatment for Metastatic Urothelial Carcinoma: A Network Meta-Analysis of Randomized Phase III Clinical Trials
Abstract
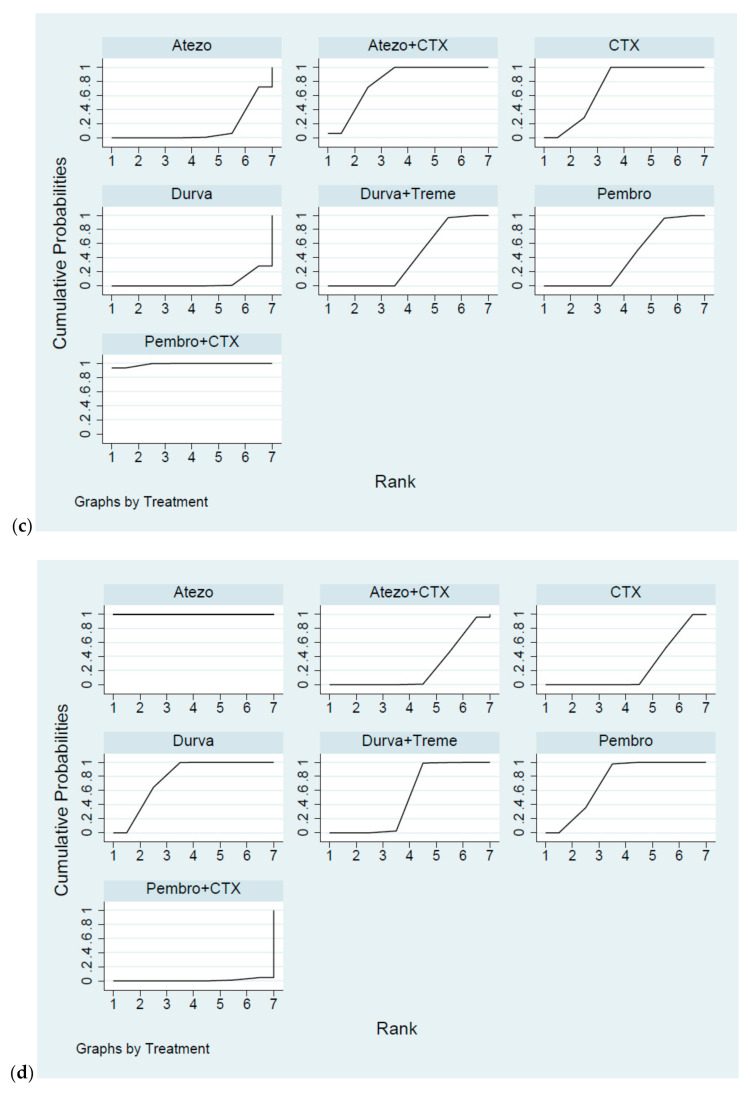
Immune checkpoints inhibitors (ICIs) were considered as second-line treatments in metastatic urothelial carcinoma (mUC) based on better survival benefit and safety profile than chemotherapy (CTX). We aimed to assess different ICIs regimens in the efficacy and safety for front-line treatments in mUC patients. A comprehensive literature search was performed and Phase II-III randomized controlled trials (RCTs) on ICIs for patients with mUC were included. The outcome was evaluated by overall survival (OS), progression of free survival (PFS), objective response rate (ORR), and grade 3-5 adverse events. Network meta-analysis was used to estimate the effect size. Surface under cumulative ranking curves (SUCRAs) were applied to rank the included treatments for each outcome. Results: The survival benefit of a single ICI was non-inferiority to chemotherapy (CTX). Although no superior effects were indicated, combination therapy (either ICIs plus CTX or ICIs plus ICIs) presented better OS compared with CTX alone. In terms of PFS, combination therapy produced a noticeable benefit over CTX. Regarding the SUCRA ranking, atezolizumab plus CTX was associated with the best ranking for OS and pembrolizumab plus CTX was the best in PFS. In terms of safety, a single ICI had better safety profile than CTX and combination therapy had a similar risk of grade 3-5 adverse events with CTX. Conclusions: Our NMA results revealed that combination therapy has better ranking compared with monotherapy in OS and acceptable AEs. ICIs alone present non-inferior OS but a lower incidence of AEs compared with CTX.
Keywords: chemotherapy; immune checkpoints inhibitors; network meta-analysis; urothelial carcinoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Nakagawa T., Taguchi S., Kanatani A., Kawai T., Ikeda M., Urakami S., Matsumoto A., Komemushi Y., Miyakawa J., Yamada D., et al. Oncologic Outcome of Metastasectomy for Urothelial Carcinoma: Who Is the Best Candidate? Ann. Surg. Oncol. 2017;24:2794–2800. doi: 10.1245/s10434-017-5970-8. - DOI - PubMed
-
- Von Der Maase H., Sengelov L., Roberts J.T., Ricci S., Dogliotti L., Oliver T., Moore M.J., Zimmermann A., Arning M. Long-Term Survival Results of a Randomized Trial Comparing Gemcitabine Plus Cisplatin, With Methotrexate, Vinblastine, Doxorubicin, Plus Cisplatin in Patients With Bladder Cancer. J. Clin. Oncol. 2005;23:4602–4608. doi: 10.1200/JCO.2005.07.757. - DOI - PubMed
-
- Loehrer P.J., Einhorn L.H., Elson P.J., Crawford E.D., Kuebler P., Tannock I., Raghavan D., Stuart-Harris R., Sarosdy M.F., A Lowe B. A randomized comparison of cisplatin alone or in combination with methotrexate, vinblastine, and doxorubicin in patients with metastatic urothelial carcinoma: A cooperative group study. J. Clin. Oncol. 1992;10:1066–1073. doi: 10.1200/JCO.1992.10.7.1066. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
