

Preoperative Detection of Liver Involvement by Right-Sided Adrenocortical Carcinoma Using CT and MRI
- PMID: 33807178
- PMCID: PMC8036813
- DOI: 10.3390/cancers13071603
Preoperative Detection of Liver Involvement by Right-Sided Adrenocortical Carcinoma Using CT and MRI
Abstract
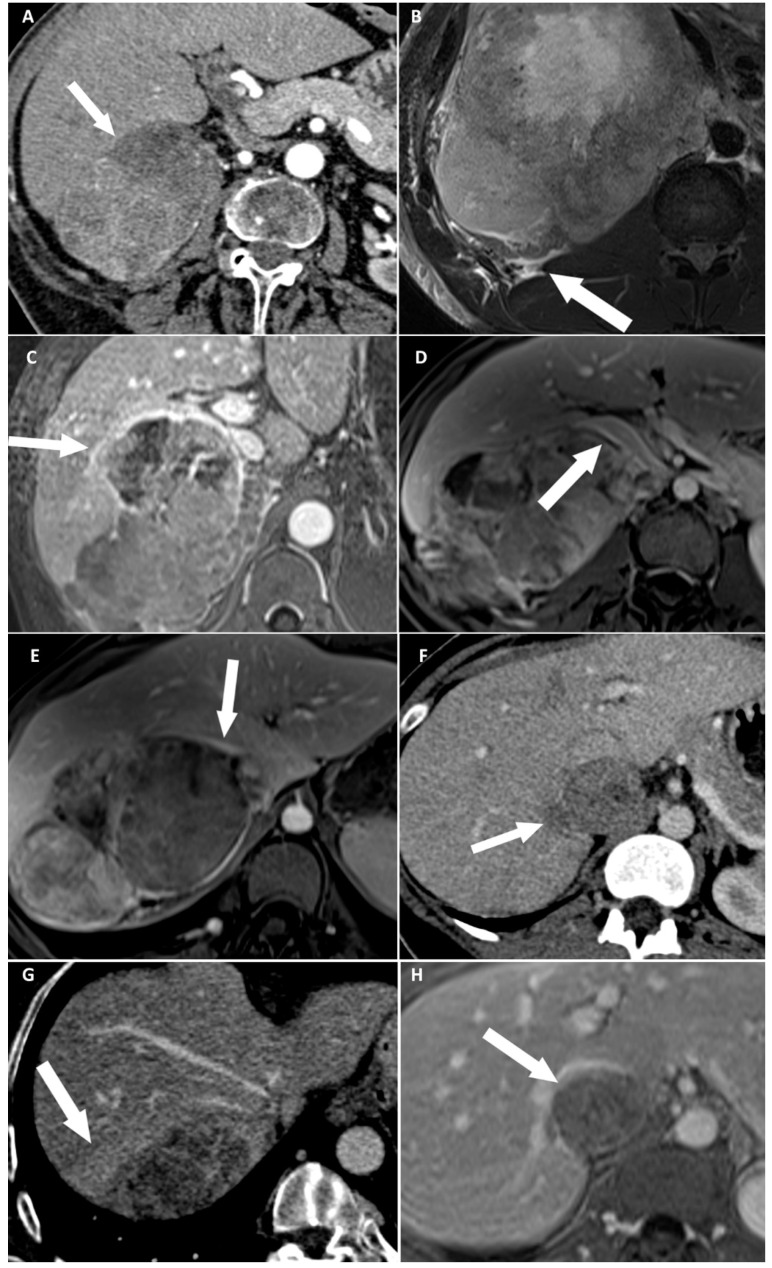
The major prognosis factor of adrenocortical carcinoma (ACC) is the completeness of surgery. The aim of our study was to identify preoperative imaging features associated with direct liver involvement (DLI) by right-sided ACC. Two radiologists, blinded to the outcome, independently reviewed preoperative CT and MRI examinations for eight signs of DLI, in patients operated for right-sided ACC and retrospectively included from November 2007 to January 2020. DLI was confirmed using surgical and histopathological findings. Kappa values were calculated. Univariable and multivariable analyses were performed by using a logistic regression model. Receiver operating characteristic (ROC) curves were built for CT and MRI. Twenty-nine patients were included. Seven patients had DLI requiring en bloc resection. At multivariable analysis, focal ACC bulge was the single independent sign associated with DLI on CT (OR: 60.00; 95% CI: 4.60-782.40; p < 0.001), and ACC contour disruption was the single independent sign associated with DLI on MRI (OR: 126.00; 95% CI: 6.82-2328.21; p < 0.001). Both signs were highly reproducible, with respective kappa values of 0.85 and 0.91. The areas under ROC curves of MRI and CT models were not different (p = 0.838). Focal ACC bulge on CT and ACC contour disruption on MRI are independent and highly reproducible signs, strongly associated with DLI by right-sided ACC on preoperative imaging. MRI does not improve the preoperative assessment of DLI by comparison with CT.
Keywords: adrenocortical carcinoma; hepatectomy; liver; neoplasm; staging.
Conflict of interest statement
The authors declare no conflict of interest related with this study.
Figures




Similar articles
-
Machine learning-based radiomics analysis of preoperative functional liver reserve with MRI and CT image.BMC Med Imaging. 2023 Jul 17;23(1):94. doi: 10.1186/s12880-023-01050-1. BMC Med Imaging. 2023. PMID: 37460944 Free PMC article.
-
Contrast-enhanced ultrasound: Improving the preoperative staging of hepatocellular carcinoma and guiding individual treatment.World J Gastroenterol. 2014 Sep 21;20(35):12628-36. doi: 10.3748/wjg.v20.i35.12628. World J Gastroenterol. 2014. PMID: 25253968 Free PMC article.
-
Association between preoperative serum albumin and prognosis in patients with adrenocortical carcinoma after primary resection: a retrospective study.BMC Cancer. 2021 Aug 26;21(1):961. doi: 10.1186/s12885-021-08689-5. BMC Cancer. 2021. PMID: 34445989 Free PMC article.
-
Surgery for adrenocortical carcinoma: When and how?Best Pract Res Clin Endocrinol Metab. 2020 May;34(3):101408. doi: 10.1016/j.beem.2020.101408. Epub 2020 Mar 3. Best Pract Res Clin Endocrinol Metab. 2020. PMID: 32265101 Review.
-
Surgical treatment of adrenal carcinoma.J Visc Surg. 2017 Oct;154(5):335-343. doi: 10.1016/j.jviscsurg.2017.06.010. Epub 2017 Jul 25. J Visc Surg. 2017. PMID: 28754418 Review.
Cited by
-
Adrenal Mass Characterization in the Era of Quantitative Imaging: State of the Art.Cancers (Basel). 2022 Jan 23;14(3):569. doi: 10.3390/cancers14030569. Cancers (Basel). 2022. PMID: 35158836 Free PMC article. Review.
-
Advances in multimodal imaging for adrenal gland disorders: integrating CT, MRI, and nuclear medicine.Jpn J Radiol. 2025 Jun;43(6):903-926. doi: 10.1007/s11604-025-01732-6. Epub 2025 Jan 11. Jpn J Radiol. 2025. PMID: 39794659 Free PMC article. Review.
References
-
- Souteiro P., Donato S., Costa C., Pereira C.A., Simões-Pereira J., Oliveira J., Belo S., Santos A.P., Cardoso H., Leite V., et al. Diagnosis, treatment, and survival analysis of adrenocortical carcinomas: A multicentric study. Hormones. 2019;19:197–203. doi: 10.1007/s42000-019-00161-1. - DOI - PubMed
-
- Abiven G., Coste J., Groussin L., Anract P., Tissier F., Legmann P., Dousset B., Bertagna X., Bertherat J. Clinical and biological features in the prognosis of adrenocortical cancer: Poor outcome of cortisol-secreting tumors in a series of 202 consecutive patients. J. Clin. Endocrinol. Metab. 2006;91:2650–2655. doi: 10.1210/jc.2005-2730. - DOI - PubMed
-
- Lughezzani G., Sun M., Perrotte P., Jeldres C., Alasker A., Isbarn H., Budaus L., Shariat S.F., Guazzoni G., Montorsi F., et al. The European Network for the Study of Adrenal Tumors staging system is prognostically superior to the International Union Against Cancer-staging system: A North American validation. Eur. J. Cancer. 2010;46:713–719. doi: 10.1016/j.ejca.2009.12.007. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
