

Locoregional Treatment of Metastatic Pancreatic Cancer Utilizing Resection, Ablation and Embolization: A Systematic Review
- PMID: 33807220
- PMCID: PMC8036519
- DOI: 10.3390/cancers13071608
Locoregional Treatment of Metastatic Pancreatic Cancer Utilizing Resection, Ablation and Embolization: A Systematic Review
Abstract
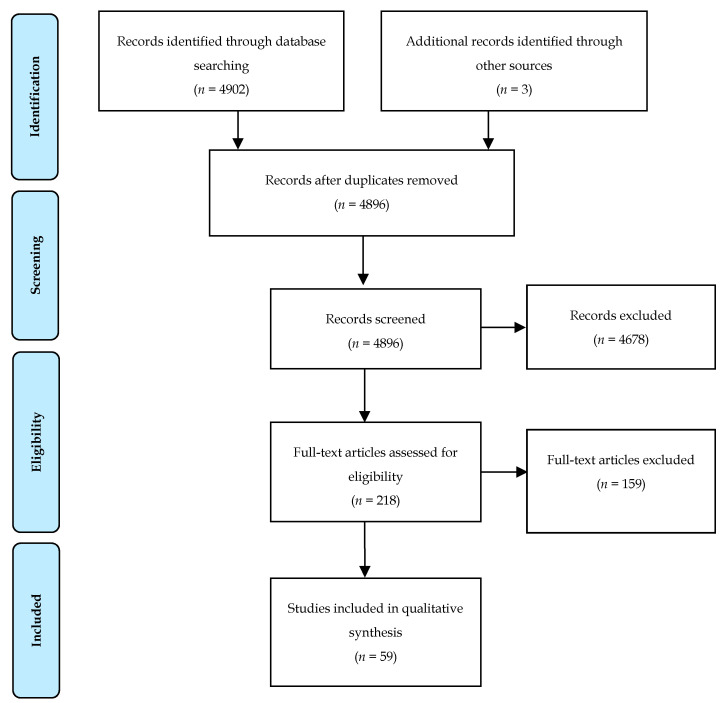
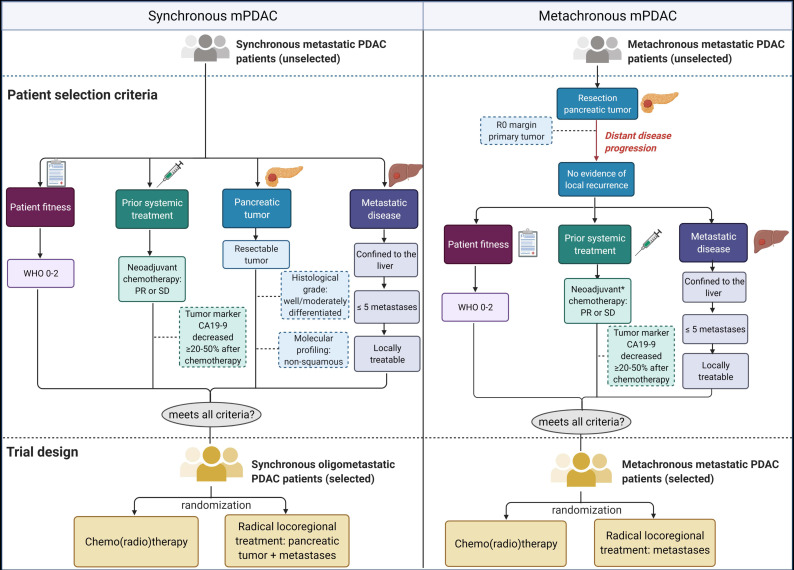
The prognosis of metastatic pancreatic ductal adenocarcinoma (mPDAC) remains universally poor, requiring new and innovative treatment approaches. In a subset of oligometastatic PDAC patients, locoregional therapy, in addition to systemic chemotherapy, may improve survival. The aim of this systematic review was to explore and evaluate the current evidence on locoregional treatments for mPDAC. A systematic literature search was conducted on locoregional techniques, including resection, ablation and embolization, for mPDAC with a focus on hepatic and pulmonary metastases. A total of 59 studies were identified, including 63,453 patients. Although subject to significant bias, radical-intent local therapy for both the primary and metastatic sites was associated with a superior median overall survival from metastatic diagnosis or treatment (hepatic mPDAC 7.8-19 months; pulmonary mPDAC 22.8-47 months) compared to control groups receiving chemotherapy or best supportive care (hepatic mPDAC 4.3-7.6 months; pulmonary mPDAC 11.8 months). To recruit patients that may benefit from these local treatments, selection appears essential. Most significant is the upfront possibility of local radical pancreatic and metastatic treatment. In addition, a patient's response to neoadjuvant systemic chemotherapy, performance status, metastatic disease load and, to a lesser degree, histological differentiation grade and tumor marker CA19-9 serum levels, are powerful prognostic factors that help identify eligible subjects. Although the exact additive value of locoregional treatments for mPDAC patients cannot be distillated from the results, locoregional primary pancreatic and metastatic treatment seems beneficial for a highly selected group of oligometastatic PDAC patients. For definite recommendations, well-designed prospective randomized controlled trials with strict in- and exclusion criteria are needed to validate these results.
Keywords: ablation; embolization; locoregional treatment; metastatic pancreatic cancer; oligo-metastases; resection.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
