

Immunological Properties of Atopic Dermatitis-Associated Alopecia Areata
- PMID: 33807704
- PMCID: PMC7961331
- DOI: 10.3390/ijms22052618
Immunological Properties of Atopic Dermatitis-Associated Alopecia Areata
Abstract
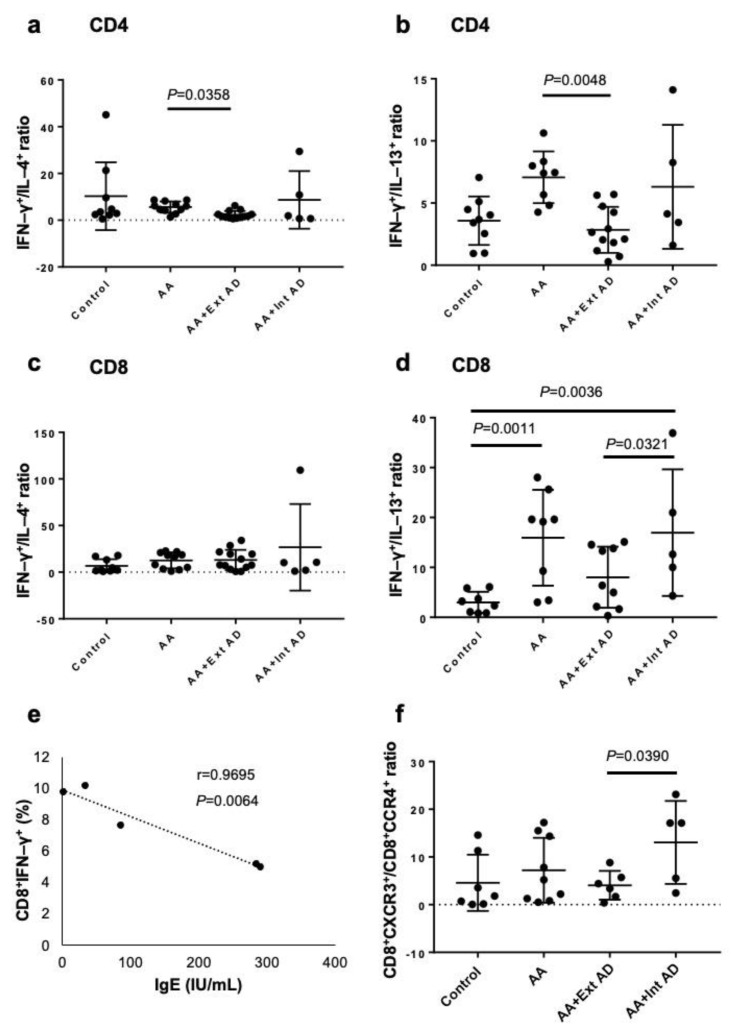
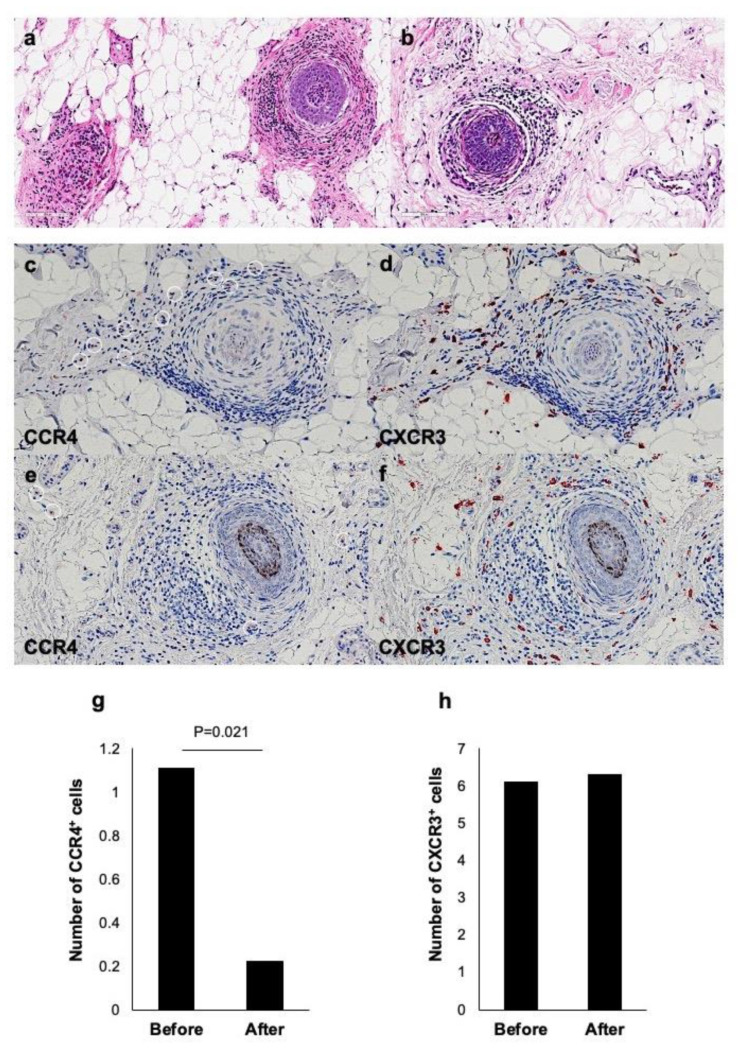
Alopecia areata (AA) is regarded as a tissue-specific and cell-mediated autoimmune disorder. Regarding the cytokine balance, AA has been considered a type 1 inflammatory disease. On the other hand, AA often complicates atopic dermatitis (AD) and AD is regarded as type 2 inflammatory disease. However, the immunological aspects of AA in relation to AD are still poorly understood. Therefore, we aim to clarify the immunological properties of AD-associated AA. In this study, we performed comparative analysis of the expression of intracytoplasmic cytokines (IFN-γ, IL-4, and IL-13), chemokine receptors (CXCR3 and CCR4) in peripheral blood which were taken from healthy controls, non-atopic AA patients, AA patients with extrinsic AD, and AA patients with intrinsic AD by flowcytometric analysis. We also compared the scalp skin samples taken from AA patients with extrinsic AD before and after treatment with dupilumab. In non-atopic AA patients, the ratios of CD4+IFN-γ+ cells to CD4+IL-4+ cells and CD4+IFN-γ+ cells to CD4+IL-13+ cells were higher than those in AA patients with extrinsic AD. Meanwhile, the ratio of CD8+IFN-γ+ cells to CD8+IL-13+ cells was significantly higher in the non-atopic AA than in the healthy controls. In AA patients with extrinsic AD, the skin AA lesion showed dense infiltration of not only CXCR3+ cells but also CCR4+ cells around hair bulb before dupilumab treatment. However, after the treatment, the number of CXCR3+ cells had no remarkable change while the number of CCR4+ cells significantly decreased. These results indicate that the immunological condition of AA may be different between atopic and non-atopic patients and between extrinsic and intrinsic AD patients. Our study provides an important notion that type 2 immunity may participate in the development of AA in extrinsic AD patients. It may be considered that the immunological state of non-atopic AA is different from that of atopic AA.
Keywords: IFN-γ; IL-13; alopecia areata; extrinsic atopic dermatitis; intrinsic atopic dermatitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
