

Endometriosis and Medical Therapy: From Progestogens to Progesterone Resistance to GnRH Antagonists: A Review
- PMID: 33807739
- PMCID: PMC7961981
- DOI: 10.3390/jcm10051085
Endometriosis and Medical Therapy: From Progestogens to Progesterone Resistance to GnRH Antagonists: A Review
Abstract
Background: The first objective of this review was to present, based on recent literature, the most frequently applied medical options (oral contraceptive pills (OCPs) and progestogens) for the management of symptomatic endometriosis, and evaluate their effectiveness in treating premenopausal women with endometriosis-associated pelvic pain, dysmenorrhea, non-menstrual pelvic pain and dyspareunia. The second objective was to review the concept of progesterone resistance and newly available treatment options.
Methods: We reviewed the most relevant papers (n = 73) on the efficacy of OCPs and progestogens as medical therapy for endometriosis, as well as those on progesterone resistance and new medical alternatives (oral gonadotropin-releasing hormone (GnRH) antagonist). Eleven papers, essentially reviews, were selected and scrutinized from among 94 papers discussing the concept of progesterone resistance.
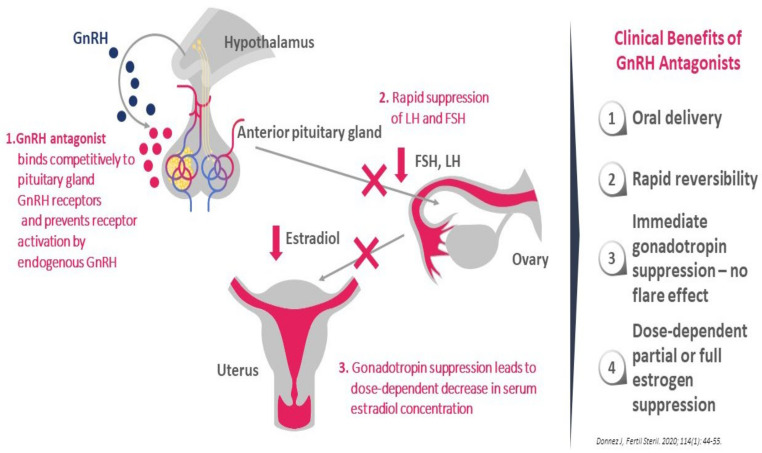
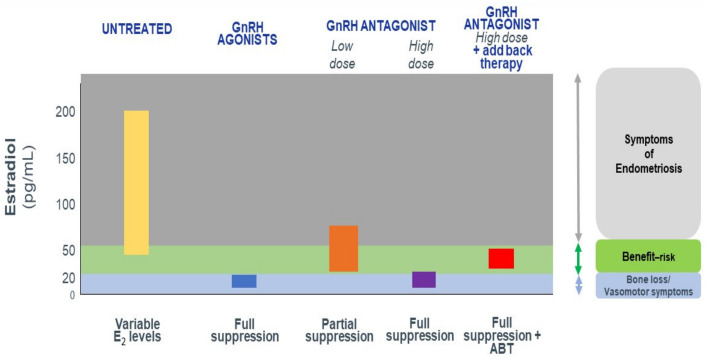
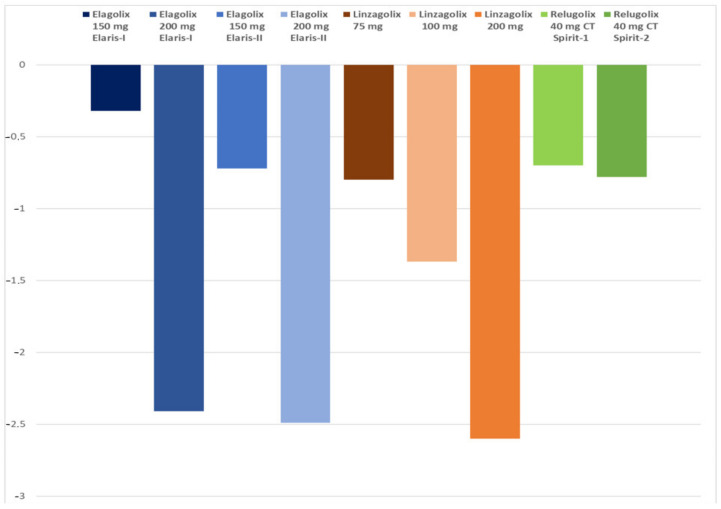
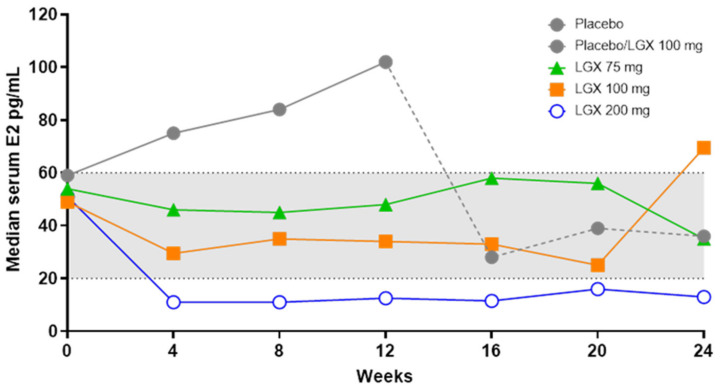
Results: Having reviewed the most significant papers, we can confirm that OCPs and progestogens are effective in two-thirds of women suffering from endometriosis, but that other options are required in case of failure (in one-third of women due to progesterone resistance) or intolerance to these compounds. It is clear that there is a need for effective long-term oral treatment capable of managing endometriosis symptoms, while mitigating the impact of side effects. Biochemical, histological and clinical evidence show that estrogens play a critical role in the pathogenesis of endometriosis, so lowering levels of circulating estrogens should be considered an effective medical approach. The efficacy of three oral GnRH antagonists is discussed on the basis of published studies.
Conclusion: There is a place for GnRH antagonists in the management of symptomatic endometriosis and clinical trials should be conducted, taking into account the different phenotypes in order to propose novel algorithms.
Keywords: GnRH antagonist; add-back therapy; dysmenorrhea; endometriosis; oral contraceptive pills; pelvic pain; progesterone resistance; progestogens.
Conflict of interest statement
Jacques Donnez is member of the Scientific Advisory Board of Obseva and Preglem. Marie Madeleine Dolmans has no conflict of interest.
Figures

Similar articles
-
GnRH Antagonists with or without Add-Back Therapy: A New Alternative in the Management of Endometriosis?Int J Mol Sci. 2021 Oct 20;22(21):11342. doi: 10.3390/ijms222111342. Int J Mol Sci. 2021. PMID: 34768770 Free PMC article. Review.
-
Profile of Linzagolix in the Management of Endometriosis, Including Design, Development and Potential Place in Therapy: A Narrative Review.Drug Des Devel Ther. 2023 Feb 8;17:369-380. doi: 10.2147/DDDT.S269976. eCollection 2023. Drug Des Devel Ther. 2023. PMID: 36789095 Free PMC article. Review.
-
A gonadotropin-releasing hormone agonist versus a low-dose oral contraceptive for pelvic pain associated with endometriosis.Fertil Steril. 1993 Jul;60(1):75-9. Fertil Steril. 1993. PMID: 8513962 Clinical Trial.
-
Uterine Fibroids and Progestogen Treatment: Lack of Evidence of Its Efficacy: A Review.J Clin Med. 2020 Dec 5;9(12):3948. doi: 10.3390/jcm9123948. J Clin Med. 2020. PMID: 33291422 Free PMC article. Review.
-
Hormonal treatment for endometriosis associated pelvic pain.Iran J Reprod Med. 2011 Summer;9(3):163-70. Iran J Reprod Med. 2011. PMID: 26396559 Free PMC article. Review.
Cited by
-
The PD-1/PD-L1 Gateway: Peripheral Immune Regulation in the Pathogenesis of Endometriosis.Int J Mol Sci. 2024 Jun 20;25(12):6775. doi: 10.3390/ijms25126775. Int J Mol Sci. 2024. PMID: 38928479 Free PMC article.
-
Genetics and Inflammation in Endometriosis: Improving Knowledge for Development of New Pharmacological Strategies.Int J Mol Sci. 2021 Aug 21;22(16):9033. doi: 10.3390/ijms22169033. Int J Mol Sci. 2021. PMID: 34445738 Free PMC article. Review.
-
Current Challenges in the Management of Chronic Pelvic Pain in Women: From Bench to Bedside.Int J Womens Health. 2022 Feb 18;14:225-244. doi: 10.2147/IJWH.S224891. eCollection 2022. Int J Womens Health. 2022. PMID: 35210869 Free PMC article. Review.
-
Research advances in drug therapy of endometriosis.Front Pharmacol. 2023 Jun 21;14:1199010. doi: 10.3389/fphar.2023.1199010. eCollection 2023. Front Pharmacol. 2023. PMID: 37416064 Free PMC article. Review.
-
Uterine Adenomyosis: From Disease Pathogenesis to a New Medical Approach Using GnRH Antagonists.Int J Environ Res Public Health. 2021 Sep 22;18(19):9941. doi: 10.3390/ijerph18199941. Int J Environ Res Public Health. 2021. PMID: 34639243 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
