

Sirolimus Pharmacokinetics Variability Points to the Relevance of Therapeutic Drug Monitoring in Pediatric Oncology
- PMID: 33808416
- PMCID: PMC8067051
- DOI: 10.3390/pharmaceutics13040470
Sirolimus Pharmacokinetics Variability Points to the Relevance of Therapeutic Drug Monitoring in Pediatric Oncology
Abstract
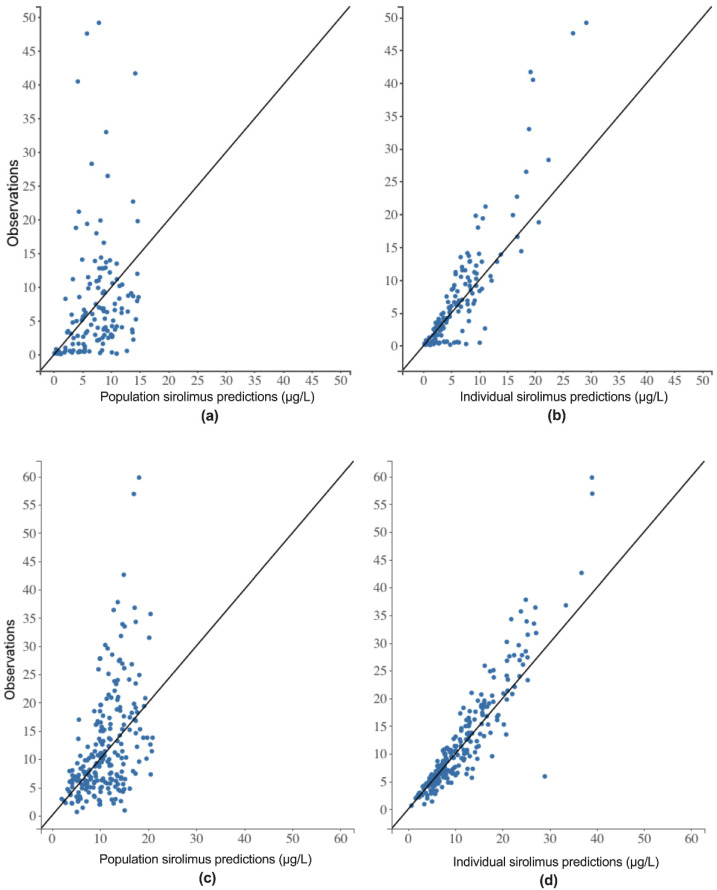
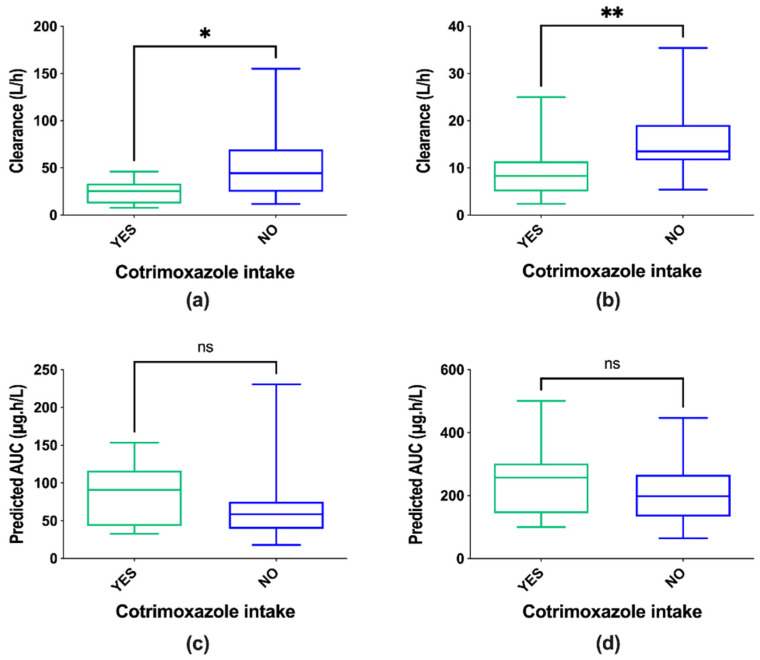
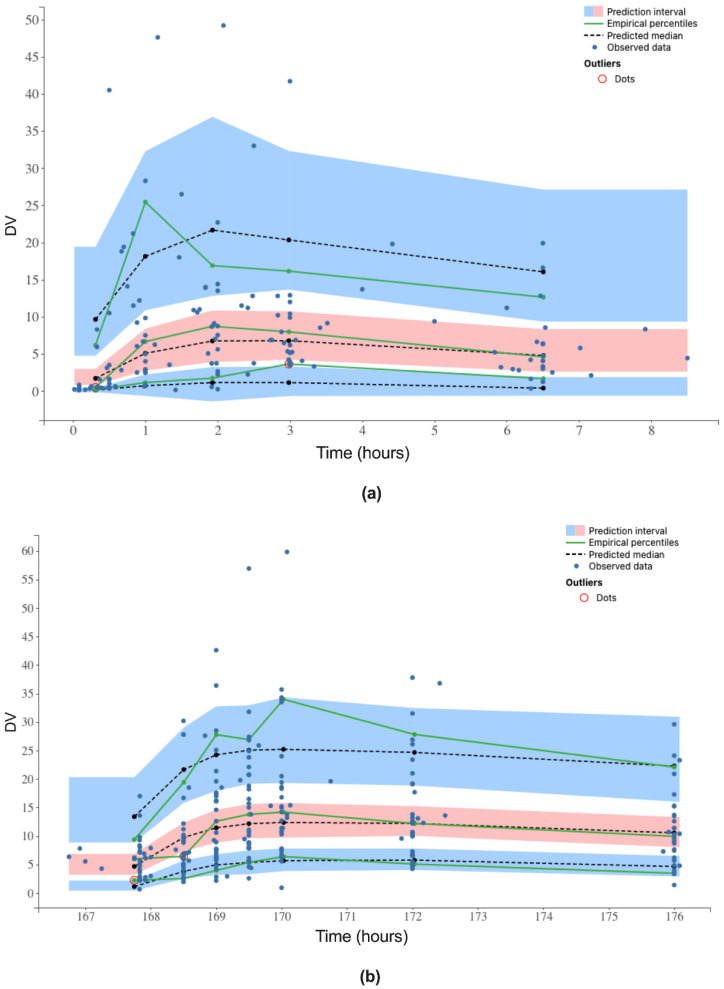
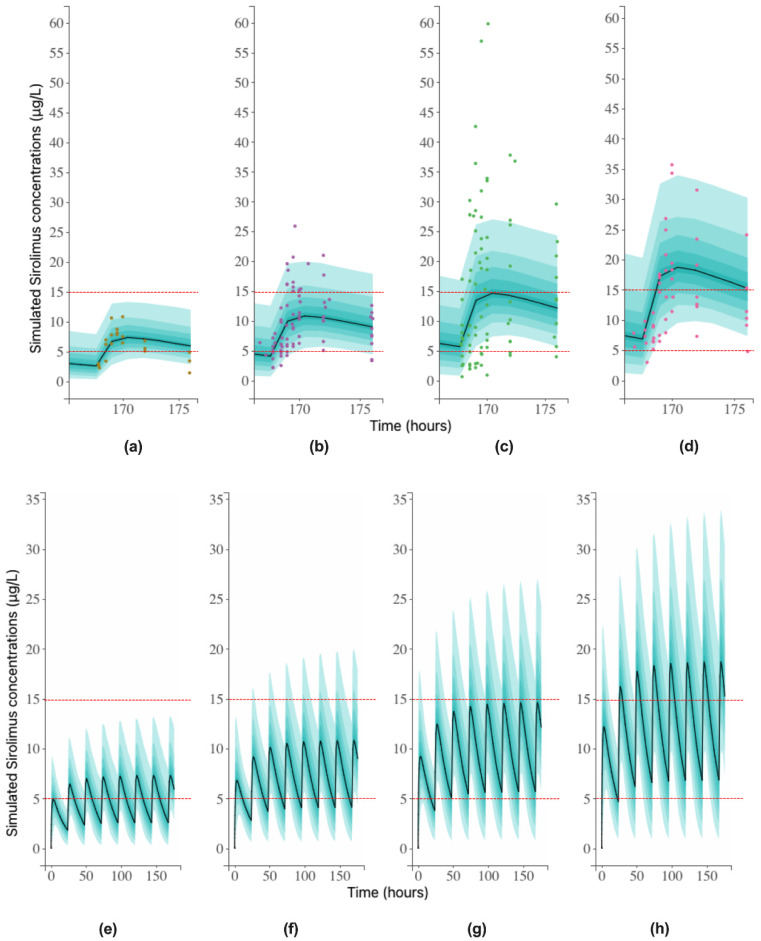
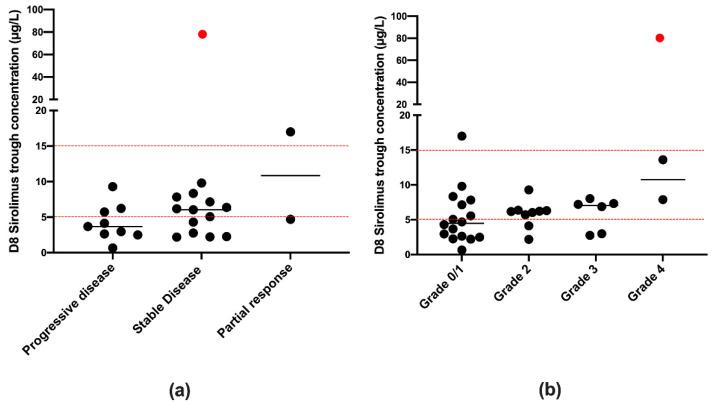
Sirolimus is widely used in transplantation, where its therapeutic drug monitoring (TDM) is well established. Evidence of a crucial role for sirolimus in the PI3K/AkT/mTor pathway has stimulated interest in its involvement in neoplasia, either as monotherapy or in combination with other antineoplastic agents. However, in cancer, there is no consensus on sirolimus TDM. In the RAPIRI phase I trial, the combination sirolimus + irinotecan was evaluated as a new treatment for refractory pediatric cancers. Blood sampling at first sirolimus intake (D1) and at steady state (D8), followed by LC/MS2 analysis, was used to develop a population pharmacokinetic model (Monolix® software). A mono-compartmental model with first-order absorption and elimination best fit the data. The only covariate retained for the final model was "body surface area" (D1 and D8). The model also demonstrated that 1.5 mg/m2 would be the recommended sirolimus dose for further studies and that steady-state TDM is necessary to adjust the dosing regimen in atypical profiles (36.4% of the population). No correlation was found between sirolimus trough concentrations and efficacy and/or observed toxicities. The study reveals the relevance of sirolimus TDM in pediatric oncology as it is needed in organ transplantation.
Keywords: Monolix® software; pediatric oncology; pharmacokinetic population modeling; pharmacokinetics; sirolimus; therapeutic drug monitoring.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
