

Current Treatment Approaches and Outcomes in the Management of Rectal Cancer Above the Age of 80
- PMID: 33808512
- PMCID: PMC8078162
- DOI: 10.3390/curroncol28020132
Current Treatment Approaches and Outcomes in the Management of Rectal Cancer Above the Age of 80
Abstract
Background: The number of cases of rectal cancer in our older cohort is expected to rise with our ageing population. In this study, we analysed patterns in treatment and the long-term outcomes of patients older than 80 years with rectal cancer across a health district.
Methods: All cases of rectal cancer managed at the Illawarra Cancer Care Centre, Australia between 2006 and 2018 were analysed from a prospectively maintained database. Patients were stratified into three age groups: ≤65 years, 66-79 years and ≥80 years of age. The clinicopathological characteristics, operative and non-operative treatment approach and survival outcomes of the three groups were compared.
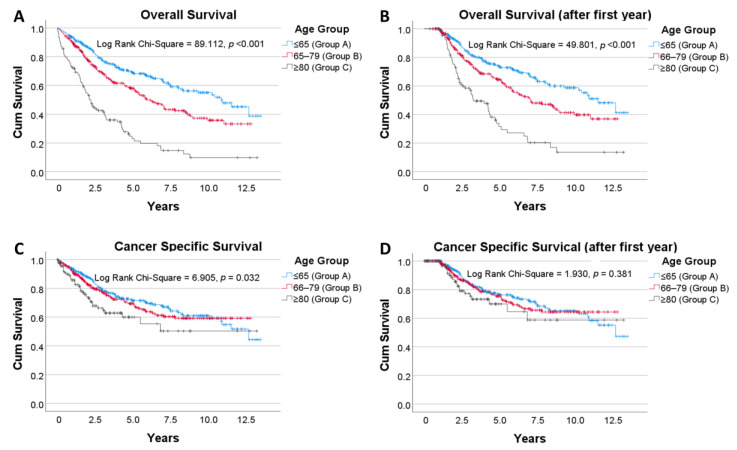
Results: Six hundred and ninety-nine patients with rectal cancer were managed, of which 118 (17%) were aged 80 and above. Patients above 80 were less likely to undergo surgery (71% vs. 90%, p < 0.001) or receive adjuvant/neoadjuvant chemoradiotherapy (p < 0.05). Of those that underwent surgical resection, their tumours were on average larger (36.5 vs. 31.5 mm, p = 0.019) and 18 mm closer the anal verge (p = 0.001). On Kaplan-Meier analysis, those above 80 had poorer cancer-specific survival when compared to their younger counterparts (p = 0.032), but this difference was no longer apparent after the first year (p = 0.381).
Conclusion: Patients above the age of 80 with rectal cancer exhibit poorer cancer-specific survival, which is accounted for in the first year after diagnosis. Priority should be made to optimise care during this period. There is a need for further research to establish the role of chemoradiotherapy in this population, which appears to be underutilised.
Keywords: aged; chemotherapy; radiotherapy; rectal neoplasms; surgery; survival.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


Similar articles
-
Fluorouracil-based adjuvant chemotherapy after preoperative chemoradiotherapy in rectal cancer: long-term results of the EORTC 22921 randomised study.Lancet Oncol. 2014 Feb;15(2):184-90. doi: 10.1016/S1470-2045(13)70599-0. Epub 2014 Jan 17. Lancet Oncol. 2014. PMID: 24440473 Clinical Trial.
-
Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): a propensity-score matched cohort analysis.Lancet Oncol. 2016 Feb;17(2):174-183. doi: 10.1016/S1470-2045(15)00467-2. Epub 2015 Dec 17. Lancet Oncol. 2016. PMID: 26705854
-
A single institution's long-term follow-up of patients with pathological complete response in locally advanced rectal adenocarcinoma following neoadjuvant chemoradiotherapy.Int J Colorectal Dis. 2017 Mar;32(3):341-348. doi: 10.1007/s00384-016-2712-5. Epub 2016 Nov 24. Int J Colorectal Dis. 2017. PMID: 27885480
-
Impact of Surgical Complications Following Resection of Locally Advanced Rectal Adenocarcinoma on Adjuvant Chemotherapy Delivery and Survival Outcomes.Dis Colon Rectum. 2016 Oct;59(10):916-24. doi: 10.1097/DCR.0000000000000659. Dis Colon Rectum. 2016. PMID: 27602922
-
Neoadjuvant chemoradiation improves oncologic outcomes in low and mid clinical T3N0 rectal cancers.Int J Colorectal Dis. 2020 Jan;35(1):77-84. doi: 10.1007/s00384-019-03452-6. Epub 2019 Nov 27. Int J Colorectal Dis. 2020. PMID: 31776698
Cited by
-
Geriatric Radiation Oncology: What We Know and What Can We Do Better?Clin Interv Aging. 2023 May 4;18:689-711. doi: 10.2147/CIA.S365495. eCollection 2023. Clin Interv Aging. 2023. PMID: 37168037 Free PMC article. Review.
-
Textbook oncologic outcomes in elderly patients undergoing neoadjuvant chemoradiotherapy and surgery for locally advanced rectal cancer: a multicenter study.Updates Surg. 2025 Aug 25. doi: 10.1007/s13304-025-02374-z. Online ahead of print. Updates Surg. 2025. PMID: 40851060
-
Geriatric Approaches to Rectal Cancer: Moving Towards a Patient-Tailored Treatment Era.J Clin Med. 2025 Feb 11;14(4):1159. doi: 10.3390/jcm14041159. J Clin Med. 2025. PMID: 40004690 Free PMC article. Review.
-
Epidemiology of cancer in older adults: a systematic review of age-related differences in solid malignancies treatment.Curr Oncol Rep. 2025 Mar;27(3):290-311. doi: 10.1007/s11912-025-01638-6. Epub 2025 Feb 15. Curr Oncol Rep. 2025. PMID: 39954206 Free PMC article.
References
-
- Safiri S., Sepanlou S.G., Ikuta K.S., Bisigano C., Salimzadeh H., Delavari A., Ansari R., Roshandel G., Merat S., Fitzmaurice C., et al. The global, regional, and national burden of colorectal cancer and its attributable risk factors in 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2019;4:913–933. doi: 10.1016/S2468-1253(19)30345-0. - DOI - PMC - PubMed
-
- Papamichael D., Audisio R.A., Glimelius B., de Gramont A., Glynne-Jones R., Haller D., Köhne C.H., Rostoft S., Lemmens V., Mitry E., et al. Treatment of colorectal cancer in older patients: International Society of Geriatric Oncology (SIOG) consensus recommendations 2013. Ann. Oncol. 2015;26:463–476. doi: 10.1093/annonc/mdu253. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
