

Diagnostic Performance of (1→3)-β-D-Glucan Alone and in Combination with Aspergillus PCR and Galactomannan in Serum of Pediatric Patients after Allogeneic Hematopoietic Stem Cell Transplantation
- PMID: 33810069
- PMCID: PMC8004996
- DOI: 10.3390/jof7030238
Diagnostic Performance of (1→3)-β-D-Glucan Alone and in Combination with Aspergillus PCR and Galactomannan in Serum of Pediatric Patients after Allogeneic Hematopoietic Stem Cell Transplantation
Abstract
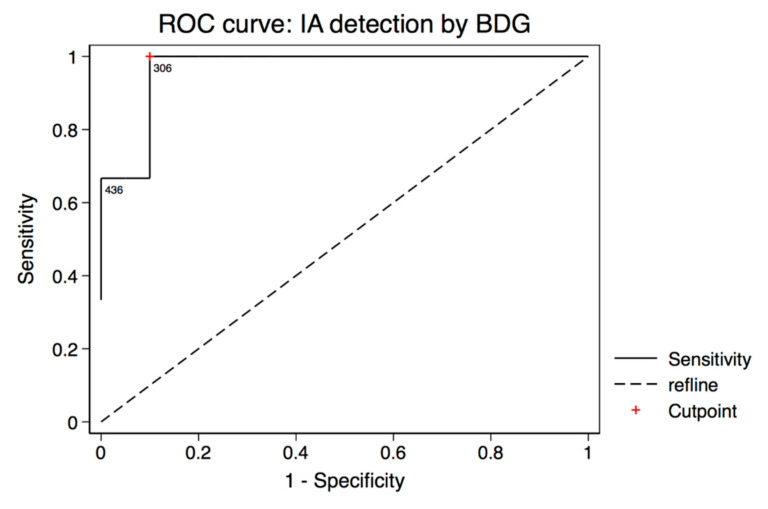
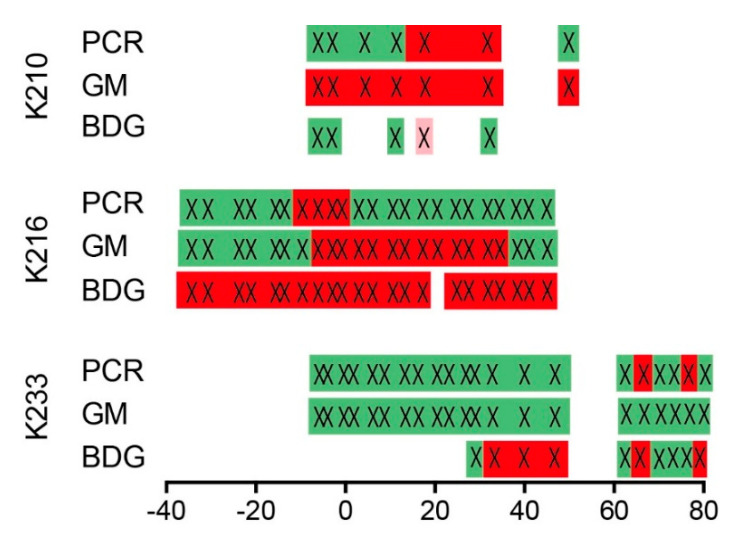
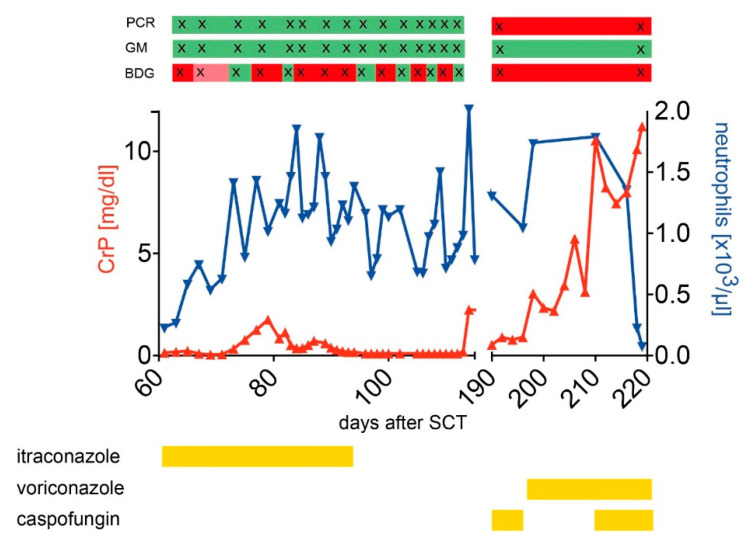
Data on biomarker-assisted diagnosis of invasive aspergillosis (IA) in pediatric patients is scarce. Therefore, we conducted a cohort study over two years including 404 serum specimens of 26 pediatric patients after allogeneic hematopoietic stem cell transplantation (alloSCT). Sera were tested prospectively twice weekly for Aspergillus-specific DNA, galactomannan (GM), and retrospectively for (1→3)-β-D-glucan (BDG). Three probable IA and two possible invasive fungal disease (IFD) cases were identified using the European Organization for Research and Treatment of Cancer and the Mycoses Study Group (EORTC/MSGERC) 2019 consensus definitions. Sensitivity and specificity for diagnosis of probable IA and possible IFD was 80% (95% confidential interval (CI): 28-99%) and 55% (95% CI: 32-77%) for BDG, 40% (95% CI: 5-85%) and 100% (95% CI: 83-100%) for GM, and 60% (95% CI: 15-95%) and 95% (95% CI: 75-100%) for Aspergillus-specific real-time PCR. However, sensitivities have to be interpreted with great caution due to the limited number of IA cases. Interestingly, the low specificity of BDG was largely caused by false-positive BDG results that clustered around the date of alloSCT. The following strategies were able to increase BDG specificity: two consecutive positive BDG tests for diagnosis (specificity 80% (95% CI: 56-94%)); using an optimized cutoff value of 306 pg/mL (specificity 90% (95% CI: 68-99%)) and testing BDG only after the acute posttransplant phase. In summary, BDG can help to diagnose IA in pediatric alloSCT recipients. However, due to the poor specificity either an increased cutoff value should be utilized or BDG results should be confirmed by an alternative Aspergillus assay.
Keywords: Aspergillus; beta-D-glucan; galactomannan; pediatric; real-time PCR.
Conflict of interest statement
J.H. received beta-D-glucan kits free of charge for other studies from Associates of Cape Cod, Inc. and from FUJIFILM Wako Chemicals Europe GmbH. The other authors declared no conflicts of interest.
Figures
Similar articles
-
Introducing 1,3-beta-d-glucan for screening and diagnosis of invasive fungal diseases in Australian high-risk haematology patients: is there a clinical benefit?Intern Med J. 2022 Mar;52(3):426-435. doi: 10.1111/imj.15046. Intern Med J. 2022. PMID: 32896984
-
Comparison of β-D-Glucan and Galactomannan in Serum for Detection of Invasive Aspergillosis: Retrospective Analysis with Focus on Early Diagnosis.J Fungi (Basel). 2020 Oct 28;6(4):253. doi: 10.3390/jof6040253. J Fungi (Basel). 2020. PMID: 33126428 Free PMC article.
-
Diagnosis of invasive fungal infections in haematological patients by combined use of galactomannan, 1,3-β-D-glucan, Aspergillus PCR, multifungal DNA-microarray, and Aspergillus azole resistance PCRs in blood and bronchoalveolar lavage samples: results of a prospective multicentre study.Clin Microbiol Infect. 2016 Oct;22(10):862-868. doi: 10.1016/j.cmi.2016.06.021. Epub 2016 Jul 5. Clin Microbiol Infect. 2016. PMID: 27393123
-
The performance of galactomannan in combination with 1,3-β-D-glucan or aspergillus-lateral flow device for the diagnosis of invasive aspergillosis: Evidences from 13 studies.Diagn Microbiol Infect Dis. 2019 Jan;93(1):44-53. doi: 10.1016/j.diagmicrobio.2018.08.005. Epub 2018 Aug 18. Diagn Microbiol Infect Dis. 2019. PMID: 30279025
-
Galactomannan and 1,3-β-d-Glucan Testing for the Diagnosis of Invasive Aspergillosis.J Fungi (Basel). 2016 Jul 4;2(3):22. doi: 10.3390/jof2030022. J Fungi (Basel). 2016. PMID: 29376937 Free PMC article. Review.
Cited by
-
Prospective Evaluation of the Fungitell® (1→3) Beta-D-Glucan Assay as a Diagnostic Tool for Invasive Fungal Disease in Pediatric Allogeneic Hematopoietic Cell Transplantation: A Report from the Children's Oncology Group.Pediatr Transplant. 2023 Feb;27(1):e14399. doi: 10.1111/petr.14399. Epub 2022 Oct 26. Pediatr Transplant. 2023. PMID: 36299233 Free PMC article.
-
Evaluation of the clinical characteristics and survival outcomes of invasive pulmonary aspergillosis patients.Front Microbiol. 2025 May 1;16:1587227. doi: 10.3389/fmicb.2025.1587227. eCollection 2025. Front Microbiol. 2025. PMID: 40376458 Free PMC article.
-
Beta-D-Glucan in Patients with Haematological Malignancies.J Fungi (Basel). 2021 Dec 7;7(12):1046. doi: 10.3390/jof7121046. J Fungi (Basel). 2021. PMID: 34947028 Free PMC article. Review.
-
Serum Beta-D-Glucan in the Diagnosis of Invasive Fungal Disease in Neonates, Children and Adolescents: A Critical Analysis of Current Data.J Fungi (Basel). 2022 Nov 30;8(12):1262. doi: 10.3390/jof8121262. J Fungi (Basel). 2022. PMID: 36547595 Free PMC article. Review.
References
-
- Kedzierska A., Kochan P., Pietrzyk A., Kedzierska J. Current status of fungal cell wall components in the immunodiagnostics of invasive fungal infections in humans: Galactomannan, mannan and (1→3)-beta-D-glucan antigens. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2007;26:755–766. doi: 10.1007/s10096-007-0373-6. - DOI - PubMed
-
- De Pauw B., Walsh T.J., Donnelly J.P., Stevens D.A., Edwards J.E., Calandra T., Pappas P.G., Maertens J., Lortholary O., Kauffman C.A., et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin. Infect. Dis. 2008;46:1813–1821. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
