

A Phase II study of autologous mesenchymal stromal cells and c-kit positive cardiac cells, alone or in combination, in patients with ischaemic heart failure: the CCTRN CONCERT-HF trial
- PMID: 33811444
- PMCID: PMC8357352
- DOI: 10.1002/ejhf.2178
A Phase II study of autologous mesenchymal stromal cells and c-kit positive cardiac cells, alone or in combination, in patients with ischaemic heart failure: the CCTRN CONCERT-HF trial
Abstract
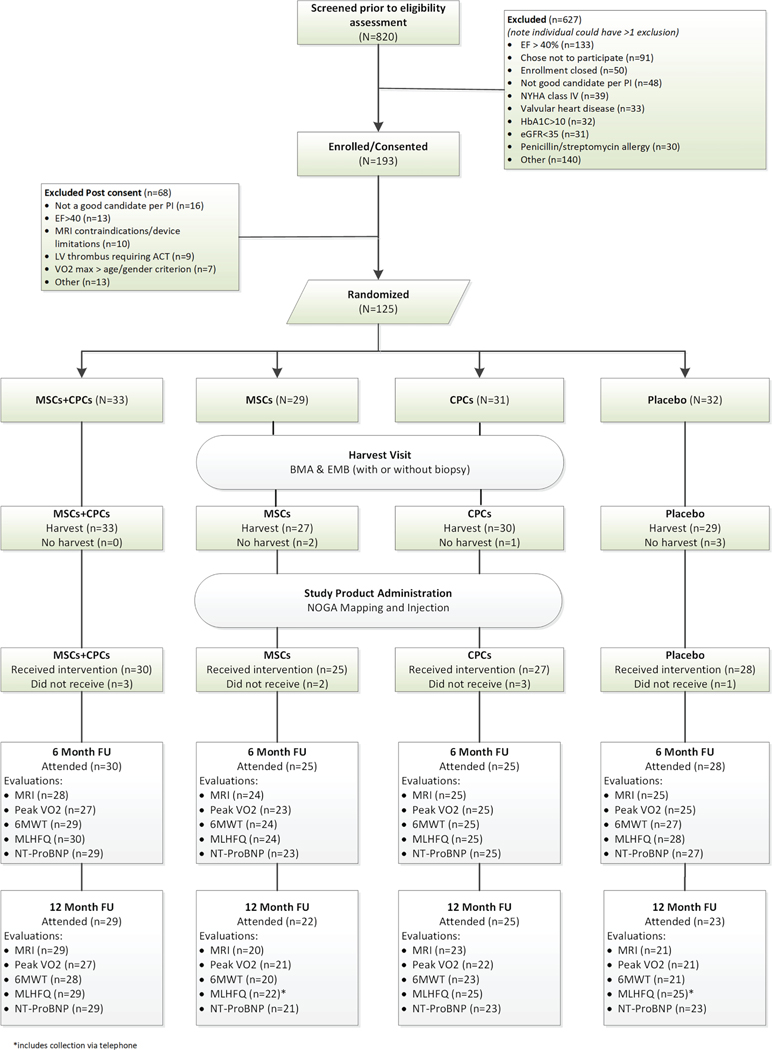
Aims: CONCERT-HF is an NHLBI-sponsored, double-blind, placebo-controlled, Phase II trial designed to determine whether treatment with autologous bone marrow-derived mesenchymal stromal cells (MSCs) and c-kit positive cardiac cells (CPCs), given alone or in combination, is feasible, safe, and beneficial in patients with heart failure (HF) caused by ischaemic cardiomyopathy.
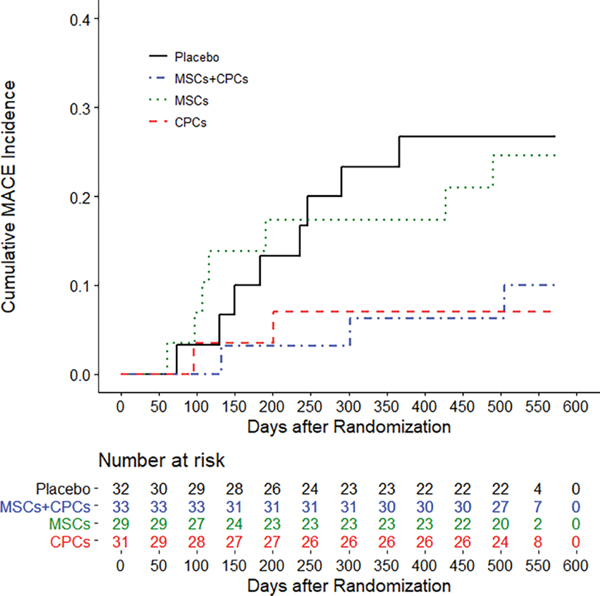
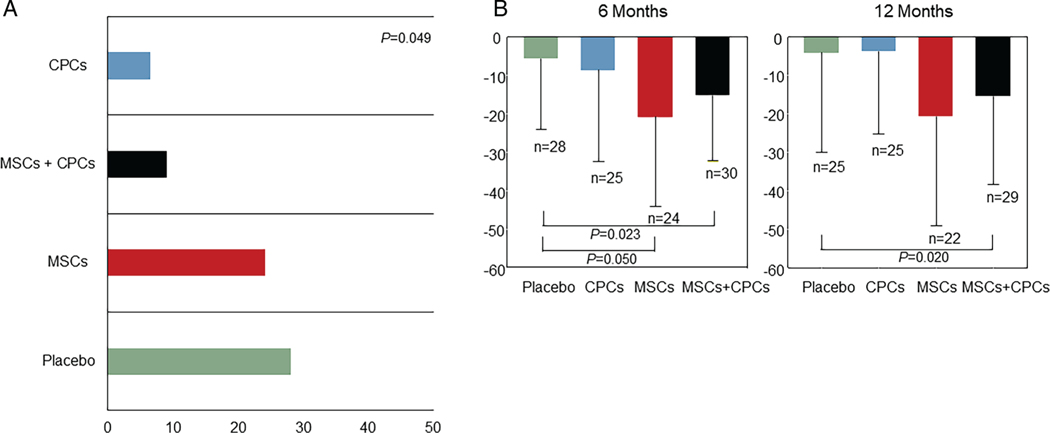
Methods and results: Patients were randomized (1:1:1:1) to transendocardial injection of MSCs combined with CPCs, MSCs alone, CPCs alone, or placebo, and followed for 12 months. Seven centres enrolled 125 participants with left ventricular ejection fraction of 28.6 ± 6.1% and scar size 19.4 ± 5.8%, in New York Heart Association class II or III. The proportion of major adverse cardiac events (MACE) was significantly decreased by CPCs alone (-22% vs. placebo, P = 0.043). Quality of life (Minnesota Living with Heart Failure Questionnaire score) was significantly improved by MSCs alone (P = 0.050) and MSCs + CPCs (P = 0.023) vs. placebo. Left ventricular ejection fraction, left ventricular volumes, scar size, 6-min walking distance, and peak oxygen consumption did not differ significantly among groups.
Conclusions: This is the first multicentre trial assessing CPCs and a combination of two cell types from different tissues in HF patients. The results show that treatment is safe and feasible. Even with maximal guideline-directed therapy, both CPCs and MSCs were associated with improved clinical outcomes (MACE and quality of life, respectively) in ischaemic HF without affecting left ventricular function or structure, suggesting possible systemic or paracrine cellular mechanisms. Combining MSCs with CPCs was associated with improvement in both these outcomes. These results suggest potential important beneficial effects of CPCs and MSCs and support further investigation in HF patients.
Keywords: Cell-based therapy; Clinical trial; Heart failure.
© 2021 European Society of Cardiology.
Conflict of interest statement
Conflict of interest:
All other authors have nothing to disclose.
Figures
Comment in
-
The CONCERT-HF trial: a sweet and sour symphony.Eur J Heart Fail. 2021 Apr;23(4):675-676. doi: 10.1002/ejhf.2188. Epub 2021 Apr 19. Eur J Heart Fail. 2021. PMID: 33840139 No abstract available.
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, Djousse L, Elkind MS, Ferguson JF, Fornage M, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Shay CM, Spartano NL, Stokes A, Tirschwell DL, VanWagner LB, Tsao; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics – 2020 update: a report from the American Heart Association. Circulation 2020;141:e139–e596. - PubMed
-
- Mathiasen AB, Qayyum AA, Jorgensen E, Helqvist S, Fischer-Nielsen A, Kofoed KF, Haack-Sorensen M, Ekblond A, Kastrup J. Bone marrow-derived mesenchymal stromal cell treatment in patients with severe ischaemic heart failure: a randomized placebo-controlled trial (MSC-HF trial). Eur Heart J 2015;36:1744–1753. - PubMed
-
- Patel AN, Henry TD, Quyyumi AA, Schaer GL, Anderson RD, Toma C, East C, Remmers AE, Goodrich J, Desai AS, Recker D, DeMaria A; ixCELL-DCM Investigators. Ixmyelocel-T for patients with ischaemic heart failure: a prospective randomised double-blind trial. Lancet 2016;387:2412–2421. - PubMed
-
- Fernández-Avilés F, Sanz-Ruiz R, Climent AM, Badimon L, Bolli R, Charron D, Fuster V, Janssens S, Kastrup J, Kim HS, Lüscher TF, Martin JF, Menasché P, Simari RD, Stone GW, Terzic A, Willerson JT, Wu JC; TACTICS (Transnational Alliance for Regenerative Therapies in Cardiovascular Syndromes) Writing Group, Authors/Task Force Members. Chairpersons, Basic Research Subcommittee, Translational Research Subcommittee, Challenges of Cardiovascular Regenerative Medicine Subcommittee, Tissue Engineering Subcommittee, Delivery, Navigation, Tracking and Assessment Subcommittee, Clinical Trials Subcommittee, Regulatory and funding strategies subcommittee, Delivery, Navigation, Tracking and Assessment Subcommittee. Global position paper on cardiovascular regenerative medicine. Eur Heart J 2017;38:2532–2546. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL087365/HL/NHLBI NIH HHS/United States
- U01 HL087318/HL/NHLBI NIH HHS/United States
- UM1 HL113460/HL/NHLBI NIH HHS/United States
- U01 HL087366/HL/NHLBI NIH HHS/United States
- F32 HL139046/HL/NHLBI NIH HHS/United States
- UM1 HL087394/HL/NHLBI NIH HHS/United States
- UM1 HL087318/HL/NHLBI NIH HHS/United States
- UM1 HL087366/HL/NHLBI NIH HHS/United States
- UM1 HL113530/HL/NHLBI NIH HHS/United States
- U01 HL087394/HL/NHLBI NIH HHS/United States
- UM1 HL113457/HL/NHLBI NIH HHS/United States
- UM1 HL087365/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
