

Specific absorption rate and temperature in neonate models resulting from exposure to a 7T head coil
- PMID: 33811667
- PMCID: PMC7614747
- DOI: 10.1002/mrm.28784
Specific absorption rate and temperature in neonate models resulting from exposure to a 7T head coil
Abstract
Purpose: To investigate safe limits for neonatal imaging using a 7T head coil, including both specific absorption rate (SAR) and temperature predictions.
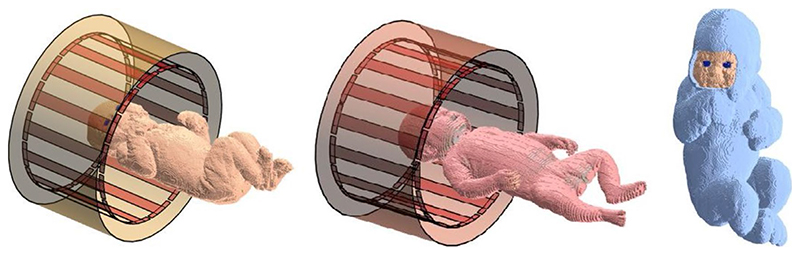
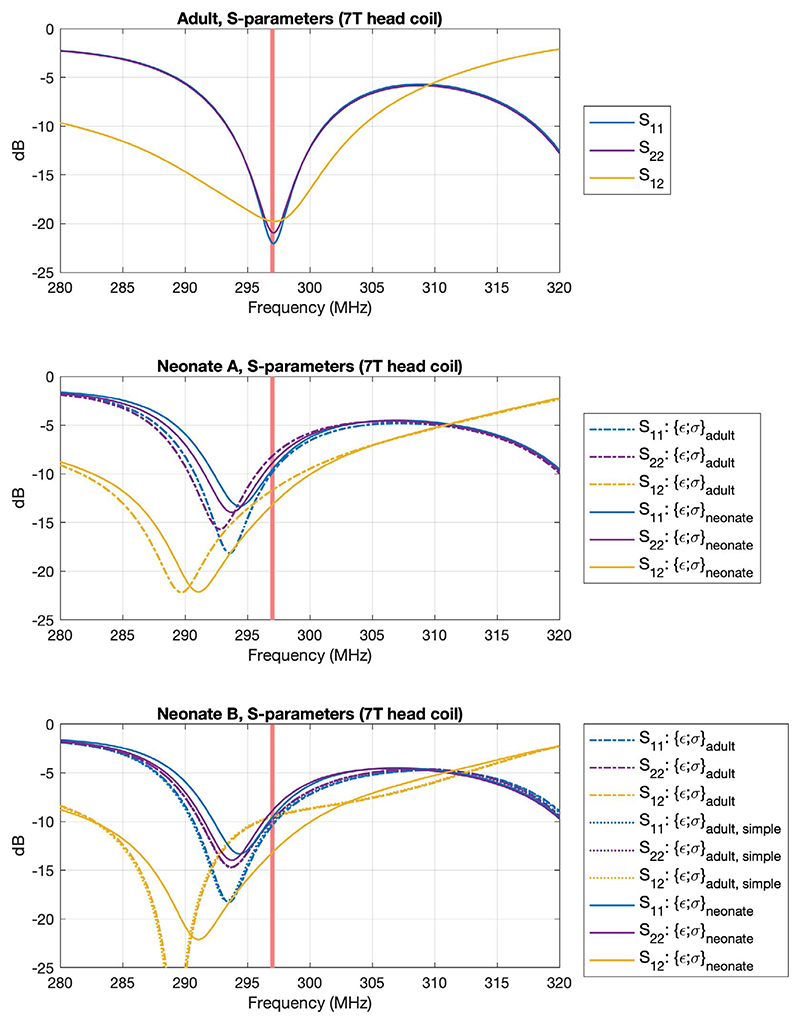
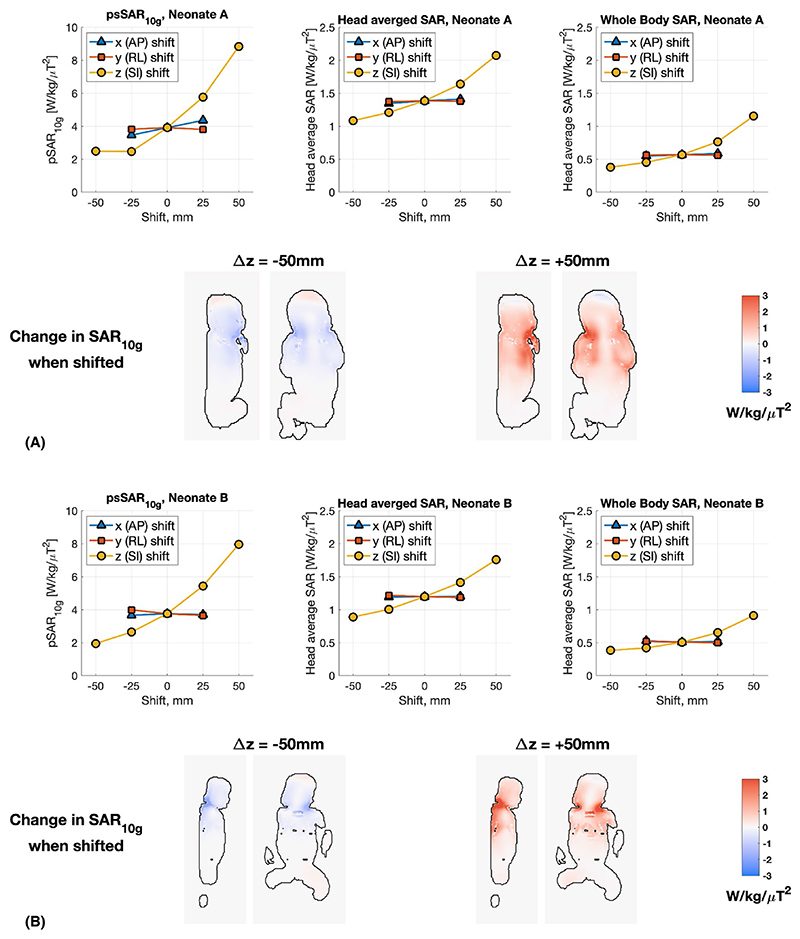
Methods: Head-centered neonate models were simulated using finite-difference time domain-based electromagnetic and thermal solvers. The effects of higher water content of neonatal tissues compared with adults, position shifts, and thermal insulation were also considered. An adult model was simulated for comparison.
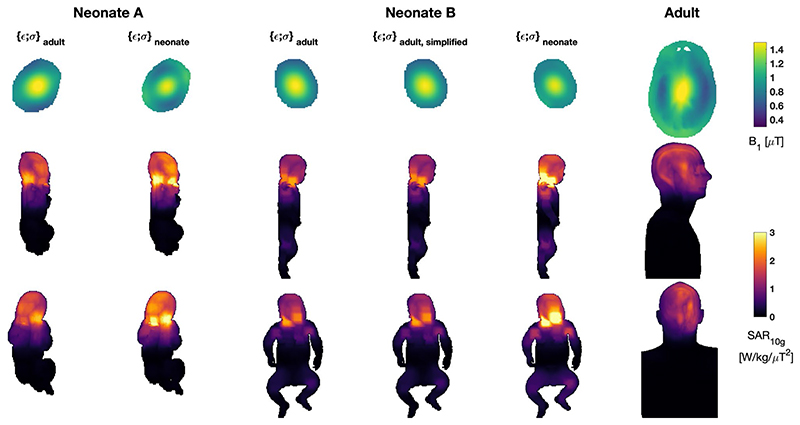
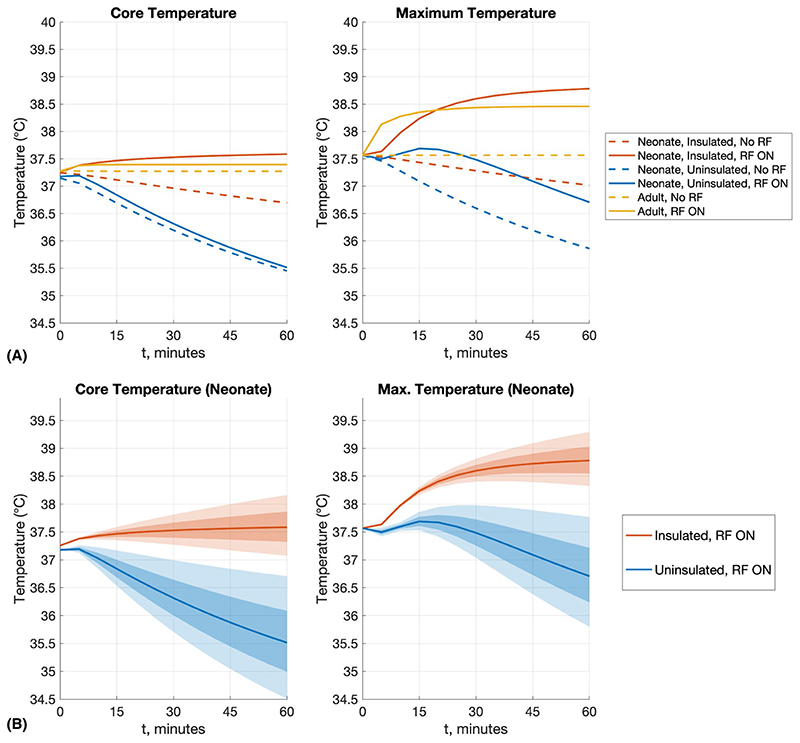
Results: Maximum and average SAR are both elevated in the neonate when compared with an adult model. When normalized to , the SAR experienced by a neonate is greater than an adult by approximately a factor of 2; when normalized to net forward power (forward-reflected), this increases to a factor of 2.5-3.0; and when normalized to absorbed power, approximately a factor of 4. Use of age-adjusted dielectric properties significantly increases the predicted SAR, compared with using adult tissue properties for the neonates. Thermal simulations predict that change in core temperature/maximum temperature remain compliant with International Electrotechnical Commission limits when a thermally insulated neonate is exposed at the SAR limit for up to an hour.
Conclusion: This study of two neonate models cannot quantify the variability expected within a larger population. Likewise, the use of age-adjusted dielectric properties have a significant effect, but while their use is well motivated by literature, there is uncertainty in the true dielectric properties of neonatal tissue. Nevertheless, the main finding is that unlike at lower field strengths, operational limits for 7T neonatal MRI using an adult head coil should be more conservative than limits for use on adults.
Keywords: 7T MRI; RF safety; neonatal imaging.
© 2021 International Society for Magnetic Resonance in Medicine.
Figures
References
-
- Kelly CJ, Hughes EJ, Rutherford MA, Counsell SJ. Advances in neonatal MRI of the brain: from research to practice. Arch Dis Child— Educ Pract Ed. 2019;104:106–110. - PubMed
-
- De Vita E, Bainbridge A, Cheong JLY, et al. Magnetic resonance imaging of neonatal encephalopathy at 4.7 Tesla: initial experiences. Pediatrics. 2006;118:e1812–e1821. - PubMed
-
- Food and Drug Administration. Guidance for Industry and Food and Drug Administration Staff— Criteria for Significant Risk Investigations of Magnetic Resonance Diagnostic Devices. 2014. [Accessed March 22, 2021]. https://www.fda.gov/regulatory-information/search-fda-guidance-documents... .
-
- International Electrotechnical Commission. IEC 60601-2-33: Medical Electrical Equipment—Particular Requirements for the Safety of Magnetic Resonance Equipment for Medical Diagnosis. 2015. [Accessed March 22, 2021]. https://webstore.iec.ch/publication/22705 .
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
