

Cancer Risk in Patients With Biopsy-Confirmed Nonalcoholic Fatty Liver Disease: A Population-Based Cohort Study
- PMID: 33811766
- PMCID: PMC10367111
- DOI: 10.1002/hep.31845
Cancer Risk in Patients With Biopsy-Confirmed Nonalcoholic Fatty Liver Disease: A Population-Based Cohort Study
Abstract
Background and aims: Recent studies link NAFLD to an increased incidence of HCC and extrahepatic cancers. However, earlier studies were small or lacked liver histology, which remains the gold standard for staging NAFLD severity.
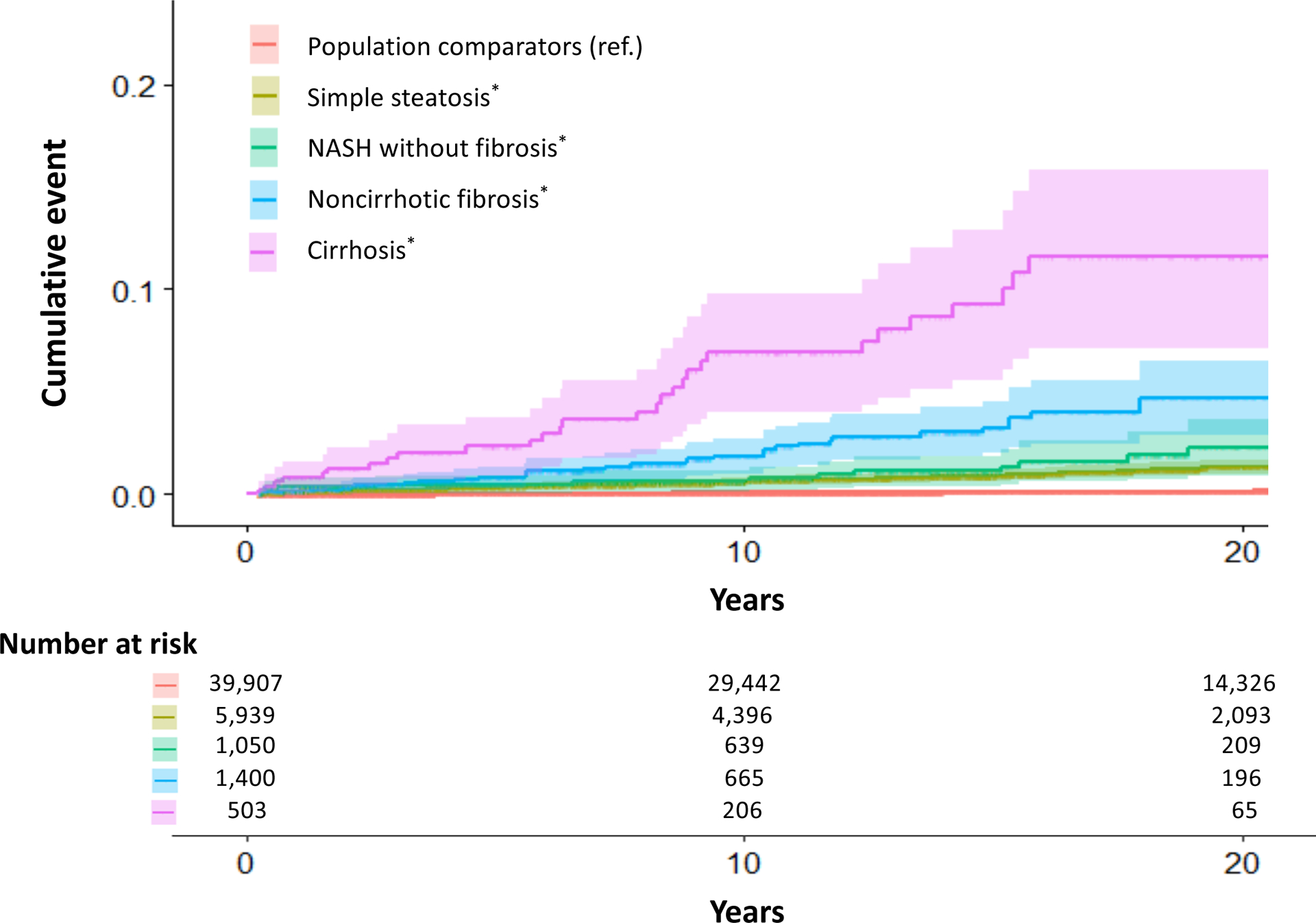
Approach and results: We conducted a population-based cohort study of all adults with histologically defined NAFLD in Sweden from 1966 to 2016 (N = 8,892). NAFLD was defined from prospectively recorded liver histopathology submitted to all 28 Swedish pathology departments and categorized as simple steatosis, nonfibrotic NASH, noncirrhotic fibrosis, and cirrhosis. NAFLD patients were individually matched to ≤5 general population controls without NAFLD by age, sex, calendar year, and county (N = 39,907). Using Cox proportional hazards modeling, we calculated multivariable adjusted HRs (aHRs) and 95% CIs. Over a median of 13.8 years, we documented 1,691 incident cancers among NAFLD patients and 6,733 among controls. Compared with controls, NAFLD patients had significantly increased overall cancer incidence (10.9 vs. 13.8 per 1,000 person-years [PYs]; difference = 2.9 per 1,000 PYs; aHR, 1.27 [95% CI, 1.18-1.36]), driven primarily by HCC (difference = 1.1 per 1,000 PYs; aHR, 17.08 [95% CI, 11.56-25.25]). HCC incidence rates increased monotonically across categories of simple steatosis, nonfibrotic NASH, noncirrhotic fibrosis, and cirrhosis (0.8 per 1,000 PYs, 1.2 per 1,000 PYs, 2.3 per 1,000 PYs, and 6.2 per 1,000 PYs, respectively; Ptrend < 0.01) and were further amplified by diabetes (1.2 per 1,000 PYs, 2.9 per 1,000 PYs, 7.2 per 1,000 PYs, and 15.7 per 1,000 PYs, respectively). In contrast, NAFLD was associated with modestly increased rates of pancreatic cancer, kidney/bladder cancer, and melanoma (differences = 0.2 per 1,000 PYs, 0.1 per 1,000 PYs, and 0.2 per 1,000 PYs, respectively), but no other cancers.
Conclusions: Compared with controls, patients with biopsy-proven NAFLD had significantly increased cancer incidence, attributable primarily to HCC, whereas the contribution of extrahepatic cancers was modest. Although HCC risk was highest with cirrhosis, substantial excess risk was also found with noncirrhotic fibrosis and comorbid diabetes.
© 2021 The Authors. Hepatology published by Wiley Periodicals LLC on behalf of American Association for the Study of Liver Diseases.
Conflict of interest statement
Dr. Ludvigsson coordinates an unrelated study on behalf of the Swedish Inflammatory Bowel Disease Registry (SWIBREG) that has received funding from Janssen Corporation. Dr. Simon’s institution has received grants from Amgen, and she has served as a consultant to Aetion for work unrelated to this manuscript. Dr. Hagström’s institution has received research grants from AstraZeneca, Intercept, and Gilead, and he has served on the advisory board for Bristol Myers Squibb and Gilead.
Figures

References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease: meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016;64:73–84. - PubMed
-
- Adams LA, Lindor KD. Nonalcoholic fatty liver disease. Ann Epidemiol 2007;17:863–869. - PubMed
-
- Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther 2011;34:274–285. - PubMed
-
- Taylor RS, Taylor RJ, Bayliss S, Hagström H, Nasr P, Schattenberg JM, et al. Association between fibrosis stage and outcomes of patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis. Gastroenterology 2020;158:611–1625.e12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
