

Establishing the Minimal Clinically Important Difference for the PROMIS Upper Extremity Computer Adaptive Test Version 2.0 in a Nonshoulder Hand and Upper Extremity Population
- PMID: 33812773
- PMCID: PMC8481350
- DOI: 10.1016/j.jhsa.2021.01.023
Establishing the Minimal Clinically Important Difference for the PROMIS Upper Extremity Computer Adaptive Test Version 2.0 in a Nonshoulder Hand and Upper Extremity Population
Abstract
Purpose: Our primary purpose was to calculate the minimal clinically important difference (MCID) for the Patient-Reported Outcomes Measurement Information System (PROMIS) Upper Extremity (UE) Computer Adaptive Test (CAT) version 2.0 (v2.0) for a nonshoulder hand and upper extremity population. Secondarily, we calculated the PROMIS Physical Function (PF) CAT v2.0 and the abbreviated version of the Disabilities of the Arm, Shoulder, and Hand (QuickDASH) MCID.
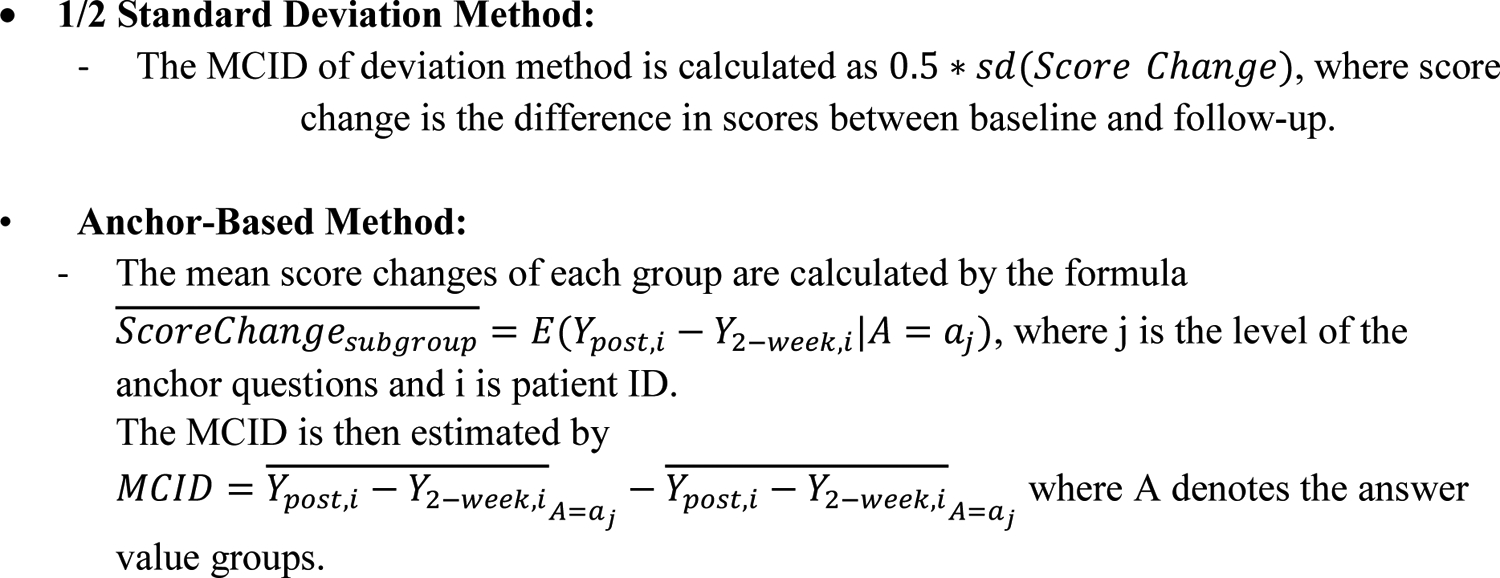
Methods: Adult patients treated by 1 of 5 fellowship-trained hand surgeons between March 2015 and September 2019 at an academic tertiary institution were identified. The PROMIS UE CAT v2.0, PROMIS PF CAT v2.0, and QuickDASH were collected via tablet computer. Inclusion required response to at least 1 of the instruments at both baseline and follow-up (6 ± 4 weeks), and a response to the anchor question: "Compared to your first evaluation at the University Orthopaedic Center, how would you describe your physical function level now?" An additional anchor question assessing treatment-related improvement was also asked. The MCID was calculated using an anchor-based approach using the mean change difference between groups reporting no change and slight change for both anchor questions, and with the 1/2 SD method.
Results: Of 2,106 participants, mean age was 48 ± 17 years, 53% were female, and 53% were recovering from surgery. Of these patients, 381 completed the PROMISE UE CAT v2.0, 497 completed the PROMIS PF CAT v2.0, and 2,018 completed the QuickDASH. The score change between baseline and follow-up was significantly different between anchor groups for both anchor-based MCID calculations. Anchor-based MCID values were 3.0 to 4.0 for the UE CAT, 2.1 to 3.6 for the PF CAT, and 10.3 for the QuickDASH. The MCID values per the 1/2 SD method were 4.1, 4.1, and 10.2, respectively.
Conclusions: We propose MCID ranges of 3.0 to 4.1 for the PROMIS UE CAT v2.0, and 2.1 to 4.1 for the PROMIS PF CAT v2.0. The observed QuickDASH MCID values (10.2-10.3) are within the range of previously published values.
Clinical relevance: These MCID estimates will aid in interpreting clinical outcomes and in powering clinical studies.
Keywords: Minimal clinically important difference (MCID); PROMIS; Physical Function (PF) CAT Version 2.0; QuickDASH/qDASH; Upper Extremity (UE) computer adaptive test (CAT) Version 2.0.
Copyright © 2021 American Society for Surgery of the Hand. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The minimal clinically important difference of the Patient-Reported Outcomes Measurement Information System (PROMIS) physical function and upper extremity computer adaptive tests and QuickDASH in the setting of elbow trauma.JSES Int. 2021 Aug 8;5(6):1132-1138. doi: 10.1016/j.jseint.2021.06.005. eCollection 2021 Nov. JSES Int. 2021. PMID: 34766096 Free PMC article.
-
The Minimal Clinically Important Difference of the PROMIS and QuickDASH Instruments in a Nonshoulder Hand and Upper Extremity Patient Population.J Hand Surg Am. 2020 May;45(5):399-407.e6. doi: 10.1016/j.jhsa.2019.12.002. Epub 2020 Jan 16. J Hand Surg Am. 2020. PMID: 31955997 Free PMC article.
-
Establishing the Substantial Clinical Benefit in a Non-Shoulder Hand and Upper Extremity Population for the QuickDASH and PROMIS Upper Extremity and Physical Function Computer Adaptive Tests.J Hand Surg Am. 2022 Apr;47(4):358-369.e3. doi: 10.1016/j.jhsa.2021.12.013. Epub 2022 Feb 23. J Hand Surg Am. 2022. PMID: 35210143 Free PMC article.
-
Minimal Clinically Important Difference of the Disabilities of the Arm, Shoulder and Hand (DASH) and the Shortened Version of the DASH (QuickDASH) in People With Musculoskeletal Disorders: A Systematic Review and Meta-Analysis.Phys Ther. 2024 May 1;104(5):pzae033. doi: 10.1093/ptj/pzae033. Phys Ther. 2024. PMID: 38438144 Free PMC article.
-
What Are the Floor and Ceiling Effects of Patient-Reported Outcomes Measurement Information System Computer Adaptive Test Domains in Orthopaedic Patients? A Systematic Review.Arthroscopy. 2020 Mar;36(3):901-912.e7. doi: 10.1016/j.arthro.2019.09.022. Epub 2020 Jan 7. Arthroscopy. 2020. PMID: 31919023
Cited by
-
FPL Reconstruction After Rupture Following Volar Plate Fixation of Distal Radius Fractures: A Case Series.J Hand Surg Glob Online. 2025 Feb 7;7(3):100693. doi: 10.1016/j.jhsg.2025.01.002. eCollection 2025 May. J Hand Surg Glob Online. 2025. PMID: 40496413 Free PMC article.
-
The minimal clinically important difference of the Patient-Reported Outcomes Measurement Information System (PROMIS) physical function and upper extremity computer adaptive tests and QuickDASH in the setting of elbow trauma.JSES Int. 2021 Aug 8;5(6):1132-1138. doi: 10.1016/j.jseint.2021.06.005. eCollection 2021 Nov. JSES Int. 2021. PMID: 34766096 Free PMC article.
-
Establishing the Minimal Clinically Important Difference and Substantial Clinical Benefit for the Pain Visual Analog Scale in a Postoperative Hand Surgery Population.J Hand Surg Am. 2022 Jul;47(7):645-653. doi: 10.1016/j.jhsa.2022.03.009. Epub 2022 May 27. J Hand Surg Am. 2022. PMID: 35644742 Free PMC article.
-
Reliability of Telephone Acquisition of the PROMIS Upper Extremity Computer Adaptive Test.J Hand Surg Am. 2021 Mar;46(3):187-199. doi: 10.1016/j.jhsa.2020.09.014. Epub 2020 Nov 24. J Hand Surg Am. 2021. PMID: 33243590 Free PMC article.
-
Minimal important change (MIC): a conceptual clarification and systematic review of MIC estimates of PROMIS measures.Qual Life Res. 2021 Oct;30(10):2729-2754. doi: 10.1007/s11136-021-02925-y. Epub 2021 Jul 10. Qual Life Res. 2021. PMID: 34247326 Free PMC article.
References
-
- Hoang-Kim A, Pegreffi F, Moroni A, Ladd A. Measuring wrist and hand function: Common scales and checklists. Injury. 2011;42(3):253–258. - PubMed
-
- Chung KC, Burns PB, Sears ED. Outcomes research in hand surgery: Where have we been and where should we go? J Hand Surg Am. 2006;31(8):1373–1379. - PubMed
-
- Hand Surgery Quality C Candidate quality measures for hand surgery. J Hand Surg Am. 2017;42(11):859–866 e853. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
