

Novel Low-Voltage MultiPulse Therapy to Terminate Atrial Fibrillation
- PMID: 33812836
- PMCID: PMC8380655
- DOI: 10.1016/j.jacep.2020.12.014
Novel Low-Voltage MultiPulse Therapy to Terminate Atrial Fibrillation
Abstract
Objectives: This first-in-human feasibility study was undertaken to translate the novel low-voltage MultiPulse Therapy (MPT) (Cardialen, Inc., Minneapolis, Minnesota), which was previously been shown to be effective in preclinical studies in terminating atrial fibrillation (AF), into clinical use.
Background: Current treatment options for AF, the most common arrhythmia in clinical practice, have limited success. Previous attempts at treating AF by using implantable devices have been limited by the painful nature of high-voltage shocks.
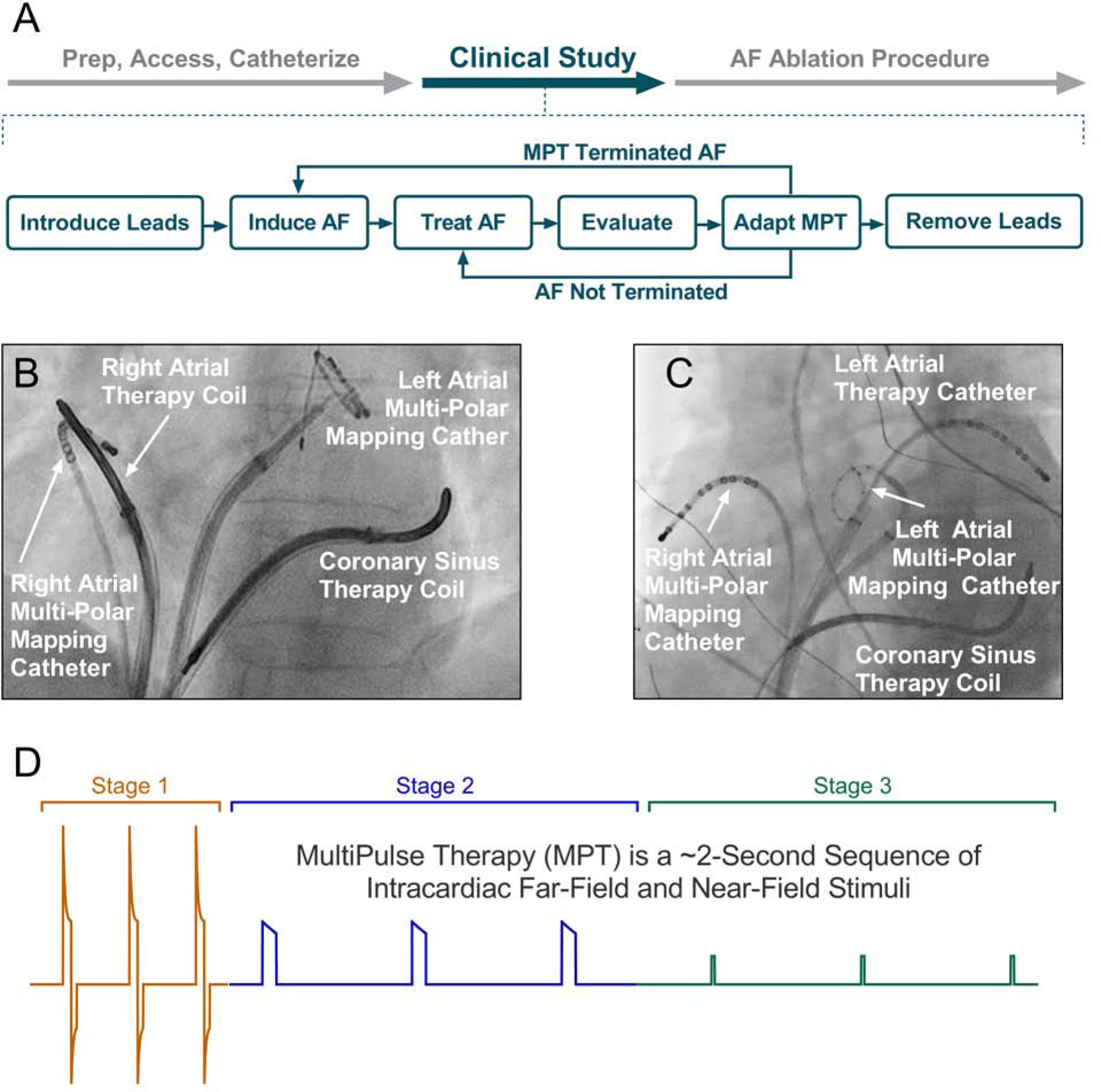
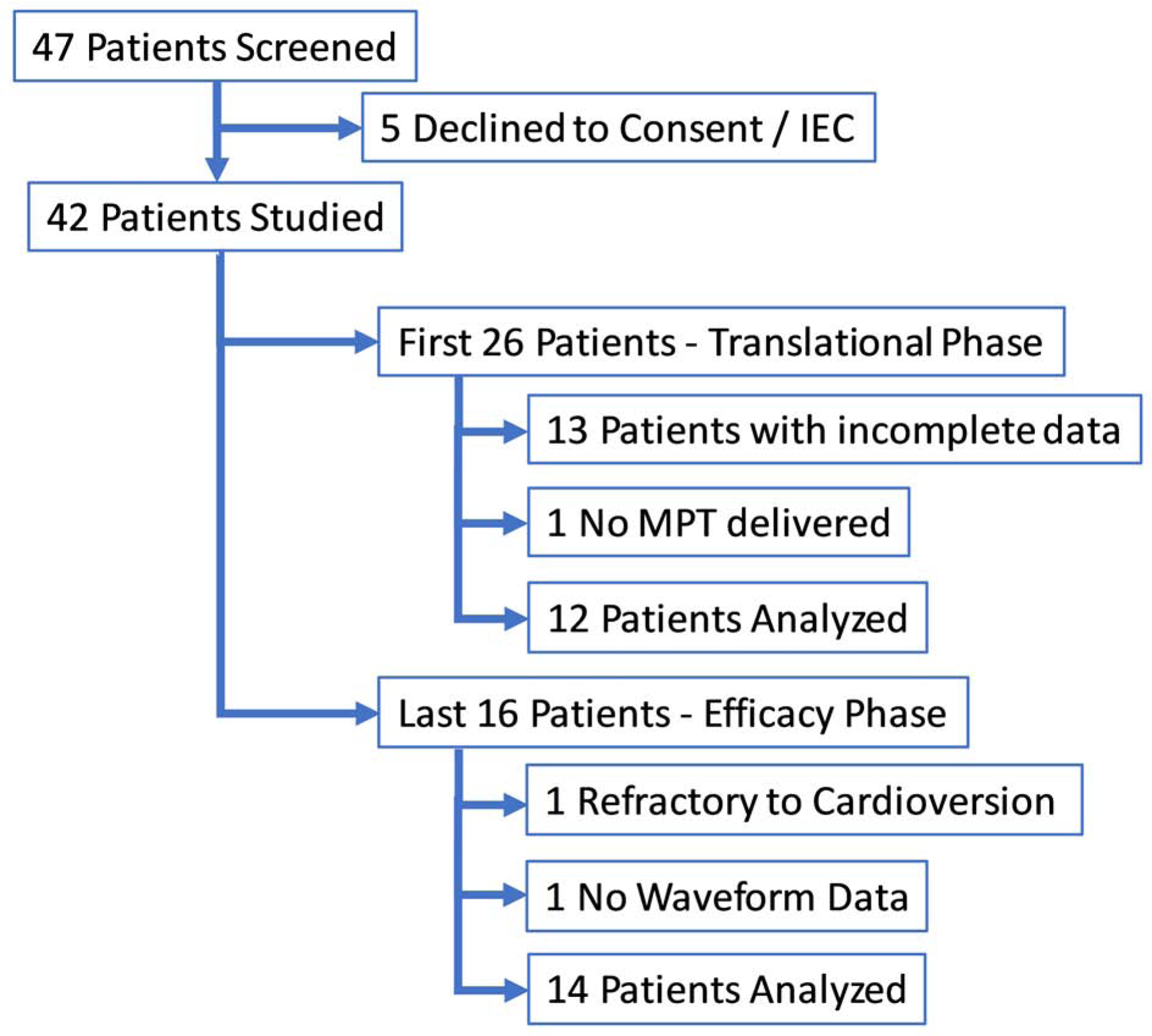
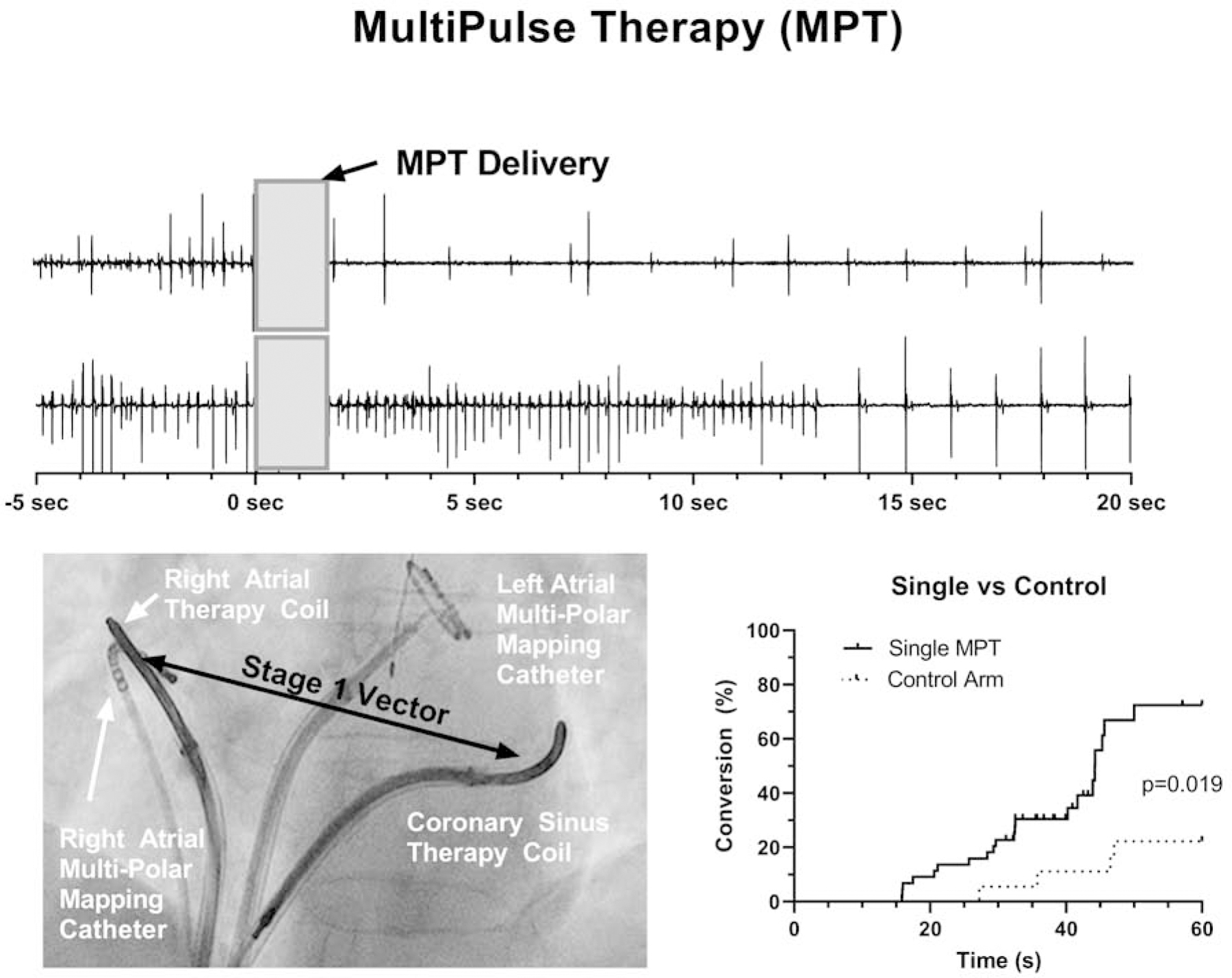
Methods: Forty-two patients undergoing AF ablation were recruited at 6 investigational centers worldwide. Before ablation, electrode catheters were placed in the coronary sinus, right and/or left atrium, for recording and stimulation. After the induction of AF, MPT, which consists of up to a 3-stage sequence of far- and near-field stimulation pulses of varied amplitude, duration, and interpulse timing, was delivered via temporary intracardiac leads. MPT parameters and delivery methods were iteratively optimized.
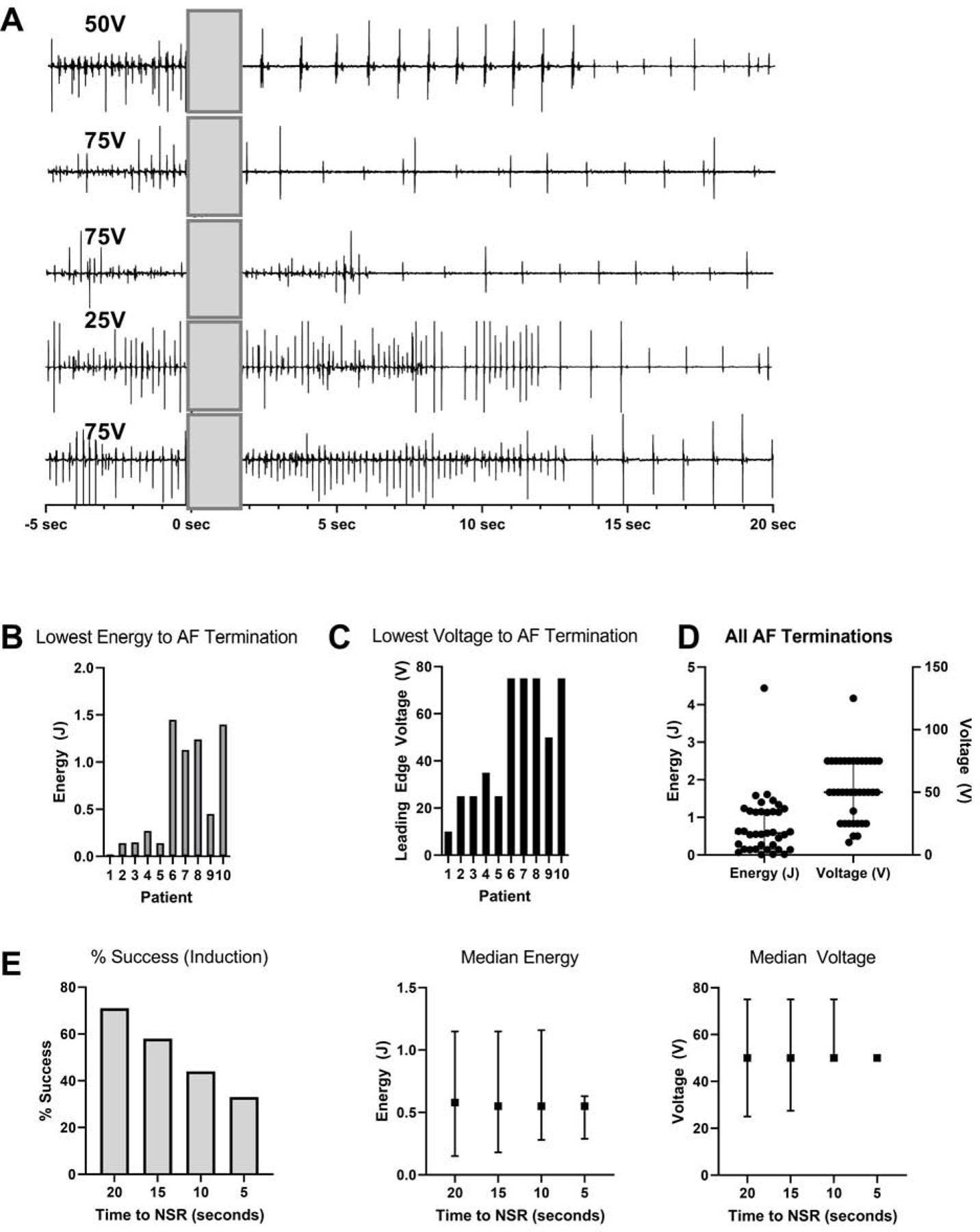
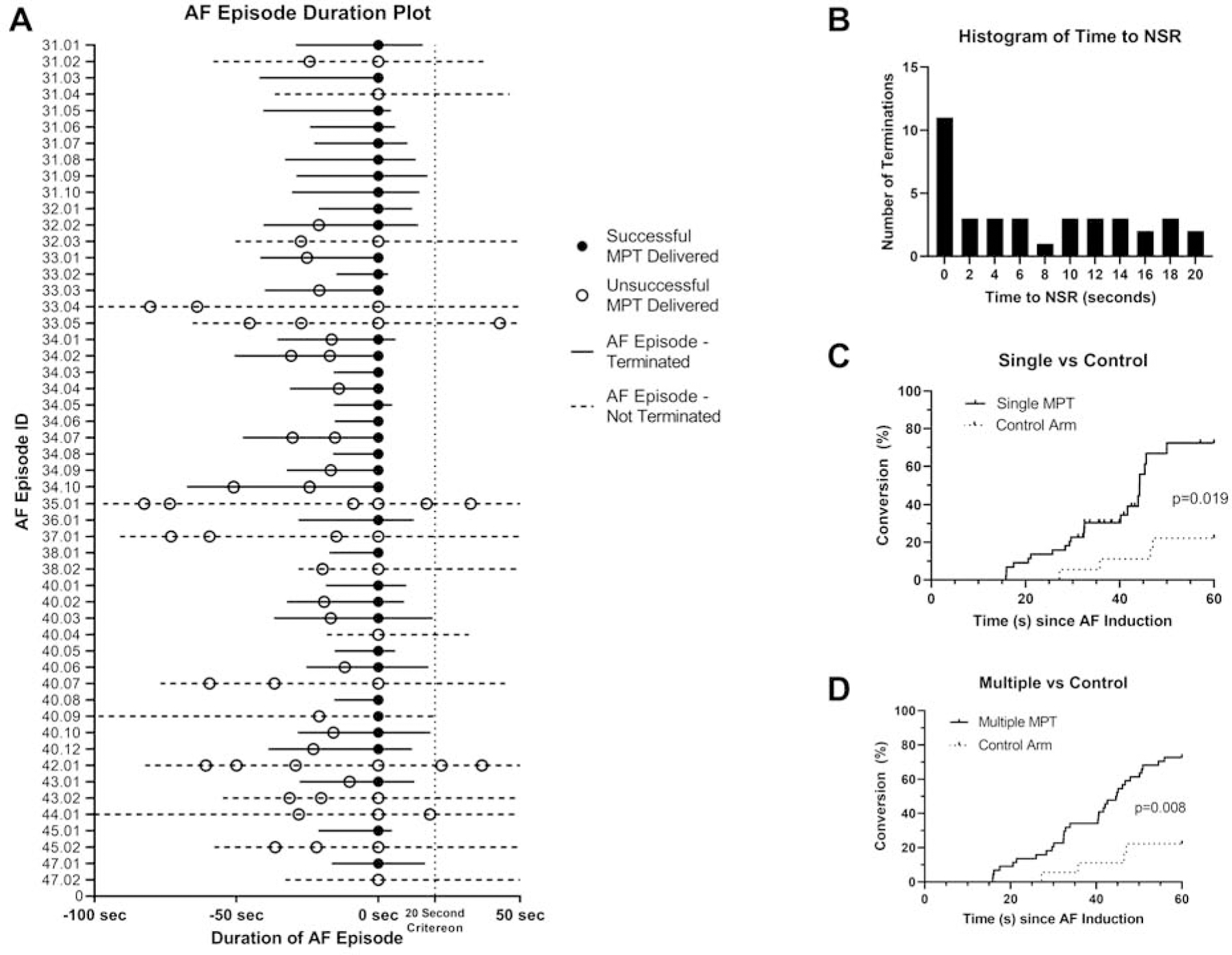
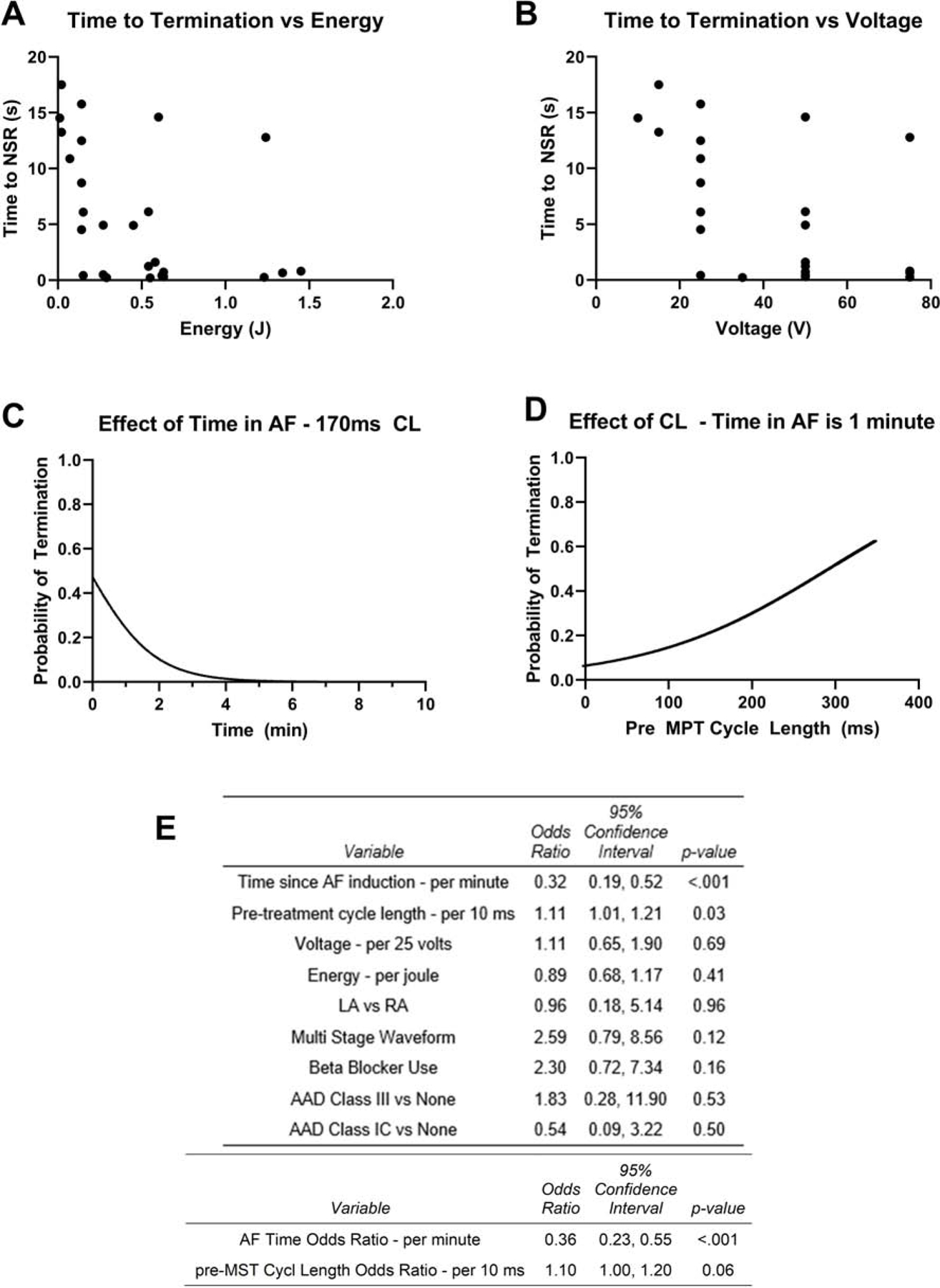
Results: In the 14 patients from the efficacy phase, MPT terminated 37 of 52 (71%) of AF episodes, with the lowest median energy of 0.36 J (interquartile range [IQR]: 0.14 to 1.21 J) and voltage of 42.5 V (IQR: 25 to 75 V). Overall, 38% of AF terminations occurred within 2 seconds of MPT delivery (p < 0.0001). Shorter time between AF induction and MPT predicted success of MPT in terminating AF (p < 0.001).
Conclusions: MPT effectively terminated AF at voltages and energies known to be well tolerated or painless in some patients. Our results support further studies of the concept of implanted devices for early AF conversion to reduce AF burden, symptoms, and progression.
Keywords: MultiPulse Therapy; atrial fibrillation; cardioversion; defibrillation.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by Cardialen Inc., Minneapolis, Minnesota; Medtronic Plc., Dublin, Ireland; and the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number 1 R43 HL107055-01. Dr. Ng was supported by the National Institute of Health Research (NIHR) (Clinical Lectureship 1716) and British Heart Foundation (RG/16/3/32175). Drs. Ng, Qureshi, and Peters were supported the Imperial College Centre for Cardiac Engineering and the NIHR Imperial Biomedical Research Centre. Drs. Ng, Mead, Peters and Efimov have or had consulting agreements with Cardialen. Mr. Shelton and Drs. Bourn and Sharma are current or former employees of Cardialen. Drs. Efimov and Peters are shareholders of Cardialen. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Low-Voltage MultiPulse Therapy: Novel, Nonpharmacological, and Nonablation Method to Terminate Atrial Fibrillation.JACC Clin Electrophysiol. 2021 Aug;7(8):1000-1002. doi: 10.1016/j.jacep.2021.01.012. JACC Clin Electrophysiol. 2021. PMID: 34412864 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
