

Evaluation of revascularization benefit quartiles using the Wound, Ischemia, and foot Infection classification system for diabetic patients with chronic limb-threatening ischemia
- PMID: 33813024
- PMCID: PMC9834912
- DOI: 10.1016/j.jvs.2021.03.017
Evaluation of revascularization benefit quartiles using the Wound, Ischemia, and foot Infection classification system for diabetic patients with chronic limb-threatening ischemia
Abstract
Objective: The Society for Vascular Surgery Wound, Ischemia, and foot Infection (WIfI) classification system was developed to stratify the risk of 1-year major amputation. Recently, the WIfI scores were used to define the estimated revascularization benefit quartiles ranging from high benefit (Q1) to questionable benefit (Q4). The aim of our study was to evaluate the revascularization benefit quartiles in a cohort of diabetic patients presenting with chronic limb-threatening ischemia (CLTI).
Methods: All diabetic patients presenting to our multidisciplinary diabetic foot and wound clinic (June 2012 to May 2020) who underwent lower extremity revascularization for CLTI were included. The affected limbs were graded using the WIfI system and assigned to an estimated benefit of revascularization quartile as previously published. One-year major amputation, complete foot healing, secondary patency, and amputation-free survival were calculated among the quartiles using Kaplan-Meier curve analyses and compared using Cox proportional hazards models.
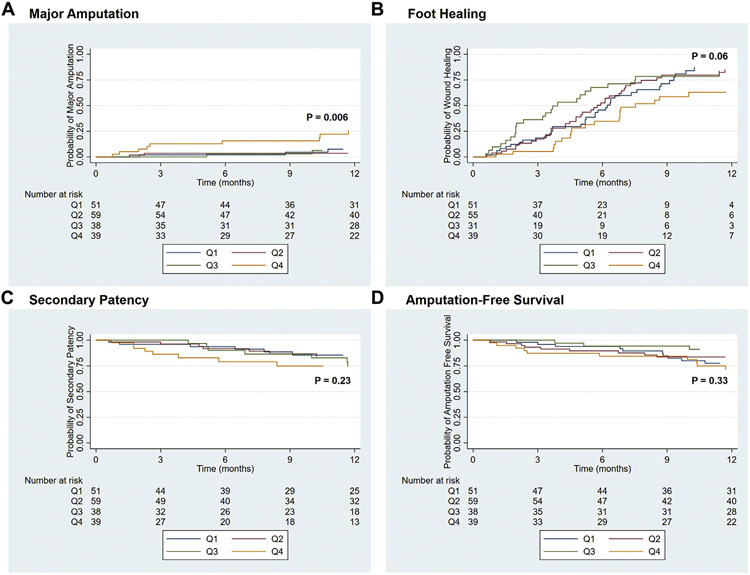
Results: Overall, 136 diabetic patients underwent revascularization of 187 limbs (mean age, 64.9 ± 11.2 years; 63.2% male; 58.8% black). The limbs were revascularized using an endovascular approach for 66.8% and open surgery for 33.2%. Of the 187 limbs, 27.3% had a high estimated benefit of revascularization (Q1), 31.6% had a moderate estimate benefit of revascularization (Q2), 20.3% had a low estimated benefit of revascularization (Q3), and 20.9% had a questionable benefit of revascularization (Q4). The estimated 1-year major amputation rates were 7.2% ± 4.1% for Q1, 3.8% ± 2.6% for Q2, 7.0% ± 4.8% for Q3, and 25.7% ± 7.5% for Q4 (P = .006). The estimated 1-year foot healing rates were 87.3% ± 5.7% for Q1, 84.8% ± 5.6% for Q2, 83.8% ± 7.4% for Q3, and 68.2% ± 9.1% for Q4 (P = .06). The overall secondary patency (P = .23) and amputation-free survival (P = .33) did not significantly differ among the groups. Using Cox proportional hazard modeling, the Q4 group had a significantly greater risk of major amputation compared with Q1 (hazard ratio, 4.26; 95% confidence interval, 1.15-15.70). Of the 14 limbs requiring major amputation, 9 (56.3%) had a patent revascularization at the time of amputation, including one of three limbs in Q1, two of two limbs in Q2, no limb in Q3, and six of nine limbs in Q4.
Conclusions: The questionable estimated revascularization benefit quartile using the WIfI classification system is significantly associated with 1-year major amputation in diabetic patients presenting with CLTI. Limbs with a questionable benefit of revascularization (Q4) will frequently require major amputation despite a patent revascularization, suggesting that the wound size and infection burden are the driving factors behind the elevated risk of major amputation in this group. Our findings support the previously described use of the WIfI classification system to predict revascularization benefit among diabetic patients with CLTI.
Keywords: Chronic limb-threatening ischemia; Diabetic foot ulcer; Revascularization benefit; WIfI.
Copyright © 2021 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author conflict of interest: none.
The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
Figures
Comment in
-
The Achilles' heel of limb salvage is the heel.J Vasc Surg. 2021 Oct;74(4):1240-1241. doi: 10.1016/j.jvs.2021.03.021. J Vasc Surg. 2021. PMID: 34598756 No abstract available.
References
-
- Mills JL Sr, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, et al. The Society for Vascular Surgery lower extremity threatened limb classification system: risk stratification based on Wound, Ischemia, and foot Infection (WIfI). J Vasc Surg 2014;59. 220–34.e1-2. - PubMed
-
- Mayor J, Chung J, Zhang Q, Montero-Baker M, Schanzer A, Conte MS, et al. Using the Society for Vascular Surgery Wound, Ischemia, and foot Infection classification to identify patients most likely to benefit from revascularization. J Vasc Surg 2019;70:776–85.e1. - PubMed
-
- Mathioudakis N, Hicks CW, Canner JK, Sherman RL, Hines KF, Lum YW, et al. The Society for Vascular Surgery Wound, Ischemia, and foot Infection (WIfI) classification system predicts wound healing but not major amputation in patients with diabetic foot ulcers treated in a multidisciplinary setting. J Vasc Surg 2017;65:1698–705.e1. - PubMed
-
- Lazarus GS, Cooper DM, Knighton DR, Percoraro RE, Rodeheaver G, Robson MC. Definitions and guidelines for assessment of wounds and evaluation of healing. Wound Repair Regen 1994;2:165–70. - PubMed
-
- Margolis DJ, Berlin JA, Strom BL. Interobserver agreement, sensitivity, and specificity of a "healed" chronic wound. Wound Repair Regen 1996;4:335–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
