

Relationship between pancreatic parenchyma loss and early postoperative hyperglycemia in patients with benign pancreatic diseases
- PMID: 33813625
- PMCID: PMC8346412
- DOI: 10.1007/s00261-021-03061-4
Relationship between pancreatic parenchyma loss and early postoperative hyperglycemia in patients with benign pancreatic diseases
Abstract
Objective: To evaluate the relationship between pancreatic parenchyma loss and early postoperative hyperglycemia in patients with benign pancreatic diseases.
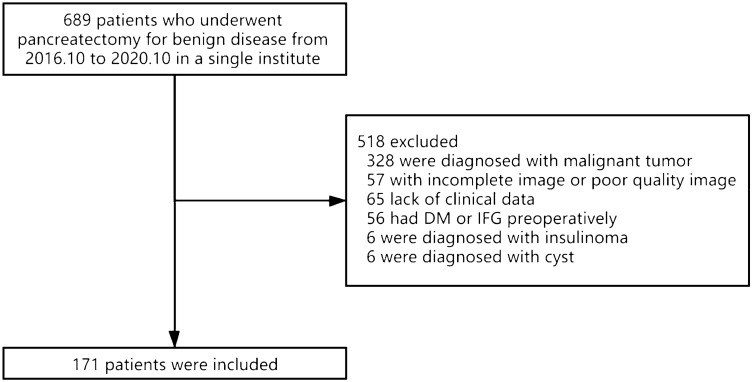
Methods: A total of 171 patients with benign pancreatic tumors or chronic pancreatitis, whose preoperative fasting blood glucose (FBG) was normal and who underwent partial pancreatectomy were reviewed. The pancreatic volume was measured by CT imaging before and after the operation. According to their different pancreatic resection volume (PRV), 171 patients were divided into five groups: < 30%, 30%-39%, 40%-49%, 50%-59%, and ≥ 60%. The correlation between the PRV and postoperative FBG was investigated. According to the postoperative FBG value, the patients were divided into a hyperglycemia group (HG) and nonhyperglycemia group (non-HG) to explore the best cutoff value of the PRV between the two groups.
Results: There were significant differences in the postoperative FBG among the five groups (PRV < 30%, 30%-39%, 40%-49%, 50%-59%, and ≥ 60%). The PRV was positively correlated with postoperative FBG in the benign tumor group and chronic pancreatitis group (R = 0.727 and 0.651, respectively). ROC curve analysis showed that the best cutoff value of the PRV between the HG (n = 84) and non-HG (n = 87) was 39.95% with an AUC = 0.898; the sensitivity was 89.29%, and the specificity was 82.76%.
Conclusion: There was a linear positive correlation between the postoperative FBG level and PRV. Patients with a PRV ≥ 40% are more likely to develop early postoperative hyperglycemia.
Keywords: CT imaging; Diabetes mellitus; Pancreatic endocrine insufficiency; Pancreatic surgery; Remnant pancreatic volume.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Teh SH, Diggs BS, Deveney CW, Sheppard BC. Patient and hospital characteristics on the variance of perioperative outcomes for pancreatic resection in the United States: a plea for outcome-based and not volume-based referral guidelines. Arch Surg. 2009;144:713–721. doi: 10.1001/archsurg.2009.67. - DOI - PubMed
-
- Ziegler KM, Nakeeb A, Pitt HA, Schmidt CM, Bishop SN, Moreno J, Matos JM, Zyromski NJ, House MG, Madura JA, Howard TJ, Lillemoe KD (2010) Pancreatic surgery: evolution at a high-volume center. Surgery 148:702-709; discussion 709-710. 10.1016/j.surg.2010.07.029 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
