

Importance of the route of insulin delivery to its control of glucose metabolism
- PMID: 33813879
- PMCID: PMC8238128
- DOI: 10.1152/ajpendo.00628.2020
Importance of the route of insulin delivery to its control of glucose metabolism
Abstract
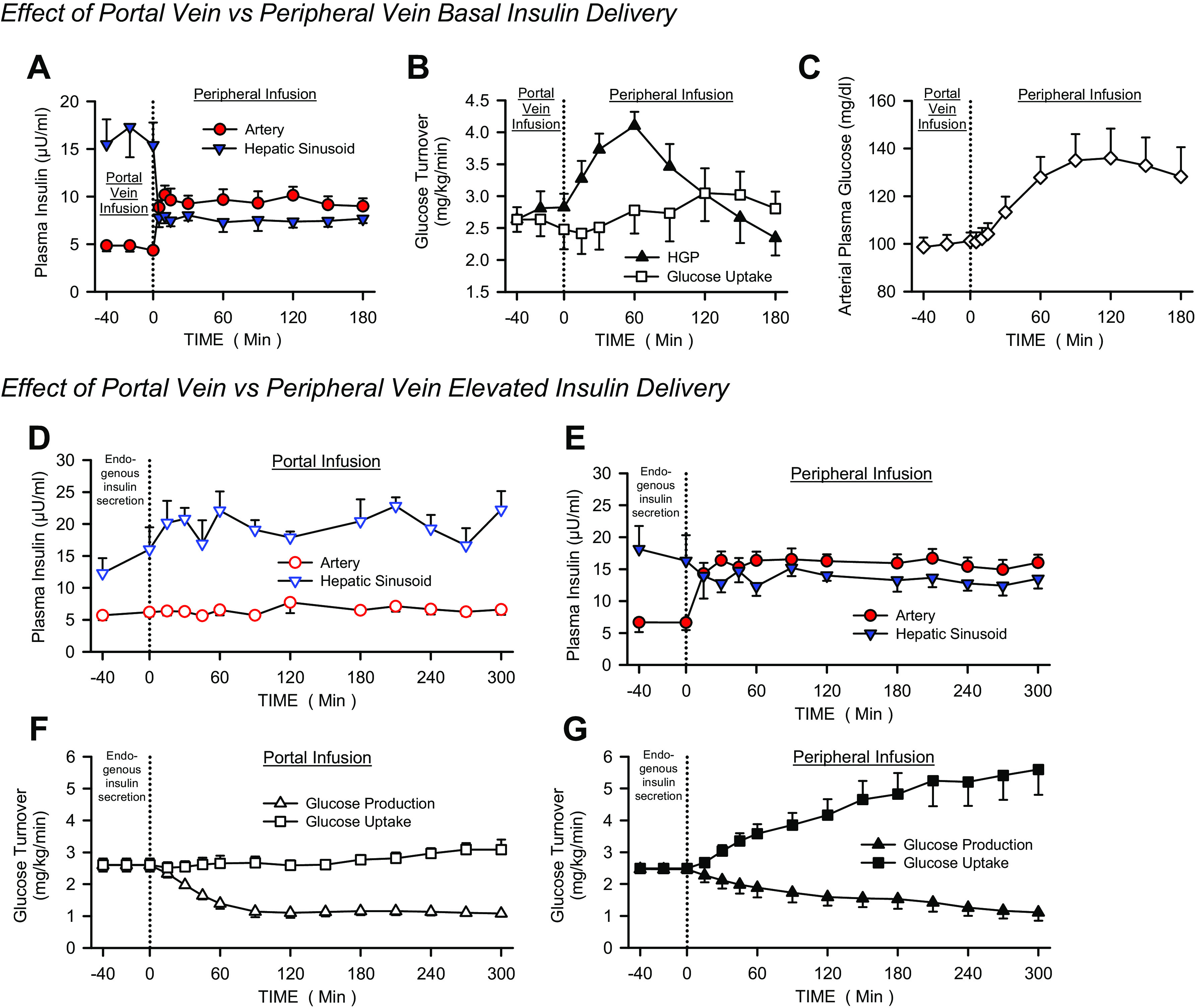
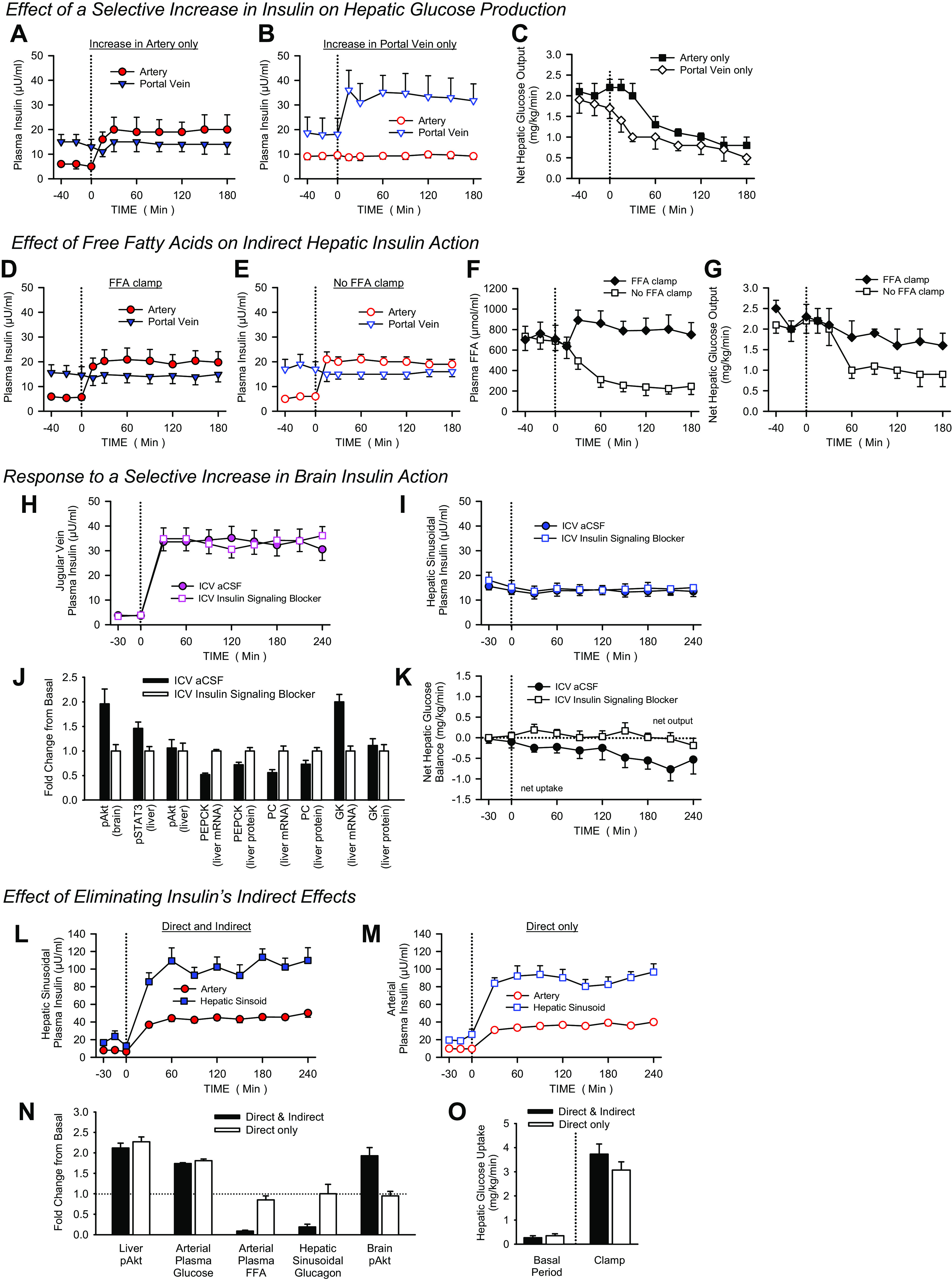
Pancreatic insulin secretion produces an insulin gradient at the liver compared with the rest of the body (approximately 3:1). This physiological distribution is lost when insulin is injected subcutaneously, causing impaired regulation of hepatic glucose production and whole body glucose uptake, as well as arterial hyperinsulinemia. Thus, the hepatoportal insulin gradient is essential to the normal control of glucose metabolism during both fasting and feeding. Insulin can regulate hepatic glucose production and uptake through multiple mechanisms, but its direct effects on the liver are dominant under physiological conditions. Given the complications associated with iatrogenic hyperinsulinemia in patients treated with insulin, insulin designed to preferentially target the liver may have therapeutic advantages.
Keywords: CNS insulin; free fatty acids; glucagon; hepatic glucose production; hepatic glucose uptake.
Conflict of interest statement
No conflict of interest for D. S. Edgerton, M. C. Moore, or G. Kraft. A. D. Cherrington has financial interests in Abvance, Biocon, Diakard/Diabetica, Fractyl, Novo Nordisk, and vTv Therapeutics.
Figures
Similar articles
-
Hyperinsulinemia compensates for infection-induced impairment in net hepatic glucose uptake during TPN.Am J Physiol Endocrinol Metab. 2000 Aug;279(2):E235-43. doi: 10.1152/ajpendo.2000.279.2.E235. Am J Physiol Endocrinol Metab. 2000. PMID: 10913021
-
Suppression of endogenous glucose production by mild hyperinsulinemia during exercise is determined predominantly by portal venous insulin.Diabetes. 2004 Feb;53(2):285-93. doi: 10.2337/diabetes.53.2.285. Diabetes. 2004. PMID: 14747277
-
Profound Sensitivity of the Liver to the Direct Effect of Insulin Allows Peripheral Insulin Delivery to Normalize Hepatic but Not Muscle Glucose Uptake in the Healthy Dog.Diabetes. 2023 Feb 1;72(2):196-209. doi: 10.2337/db22-0471. Diabetes. 2023. PMID: 36280227 Free PMC article.
-
Minimising hypoglycaemia in the real world: the challenge of insulin.Diabetologia. 2021 May;64(5):978-984. doi: 10.1007/s00125-020-05354-7. Epub 2021 Jan 16. Diabetologia. 2021. PMID: 33452892 Review.
-
Regulation of Postabsorptive and Postprandial Glucose Metabolism by Insulin-Dependent and Insulin-Independent Mechanisms: An Integrative Approach.Nutrients. 2021 Jan 6;13(1):159. doi: 10.3390/nu13010159. Nutrients. 2021. PMID: 33419065 Free PMC article. Review.
Cited by
-
Gut microbiota composition alteration analysis and functional categorization in children with growth hormone deficiency.Front Pediatr. 2023 Feb 24;11:1133258. doi: 10.3389/fped.2023.1133258. eCollection 2023. Front Pediatr. 2023. PMID: 36911039 Free PMC article.
-
Insulin Therapy for the Management of Diabetes Mellitus: A Narrative Review of Innovative Treatment Strategies.Diabetes Ther. 2023 Nov;14(11):1801-1831. doi: 10.1007/s13300-023-01468-4. Epub 2023 Sep 22. Diabetes Ther. 2023. PMID: 37736787 Free PMC article. Review.
-
Delivery of biologics: Topical administration.Biomaterials. 2023 Nov;302:122312. doi: 10.1016/j.biomaterials.2023.122312. Epub 2023 Sep 4. Biomaterials. 2023. PMID: 37690380 Free PMC article. Review.
-
Dual-hormone artificial pancreas for management of type 1 diabetes: Recent progress and future directions.Artif Organs. 2021 Sep;45(9):968-986. doi: 10.1111/aor.14023. Epub 2021 Jul 15. Artif Organs. 2021. PMID: 34263961 Free PMC article. Review.
-
Morning Engagement of Hepatic Insulin Receptors Improves Afternoon Hepatic Glucose Disposal and Storage.bioRxiv [Preprint]. 2024 Sep 27:2024.09.25.614969. doi: 10.1101/2024.09.25.614969. bioRxiv. 2024. Update in: Diabetes. 2025 Mar 01;74(3):270-281. doi: 10.2337/db24-0786. PMID: 39386695 Free PMC article. Updated. Preprint.
References
-
- Aronoff SL, Berkowitz K, Shreiner B, Want L. Glucose metabolism and regulation: beyond insulin and glucagon. Diabetes Spectrum 17: 183–190, 2004. doi:10.2337/DIASPECT.17.3.183. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical