

Risk stratification of cardiac metastases using late gadolinium enhancement cardiovascular magnetic resonance: prognostic impact of hypo-enhancement evidenced tumor avascularity
- PMID: 33814005
- PMCID: PMC8020547
- DOI: 10.1186/s12968-021-00727-2
Risk stratification of cardiac metastases using late gadolinium enhancement cardiovascular magnetic resonance: prognostic impact of hypo-enhancement evidenced tumor avascularity
Abstract
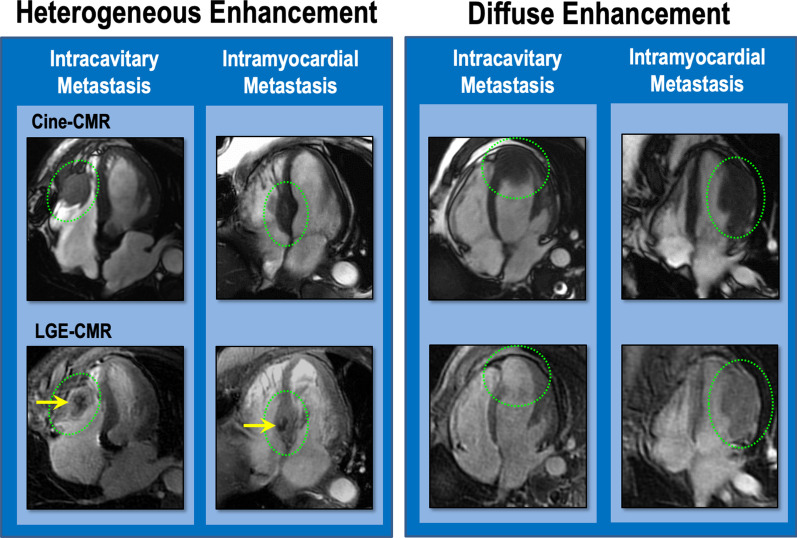
Background: Late gadolinium enhancement (LGE) cardiovascular magnetic resonance (CMR) is widely used to identify cardiac neoplasms, for which diagnosis is predicated on enhancement stemming from lesion vascularity: Impact of contrast-enhancement pattern on clinical outcomes is unknown. The objective of this study was to determine whether cardiac metastasis (CMET) enhancement pattern on LGE-CMR impacts prognosis, with focus on heterogeneous lesion enhancement as a marker of tumor avascularity.
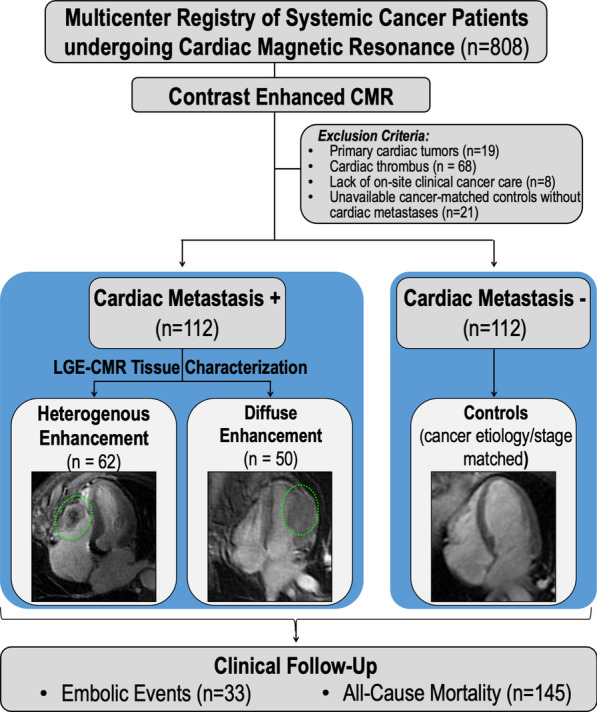
Methods: Advanced (stage IV) systemic cancer patients with and without CMET matched (1:1) by cancer etiology underwent a standardized CMR protocol. CMET was identified via established LGE-CMR criteria based on lesion enhancement; enhancement pattern was further classified as heterogeneous (enhancing and non-enhancing components) or diffuse and assessed via quantitative (contrast-to-noise ratio (CNR); signal-to-noise ratio (SNR)) analyses. Embolic events and mortality were tested in relation to lesion location and contrast-enhancement pattern.
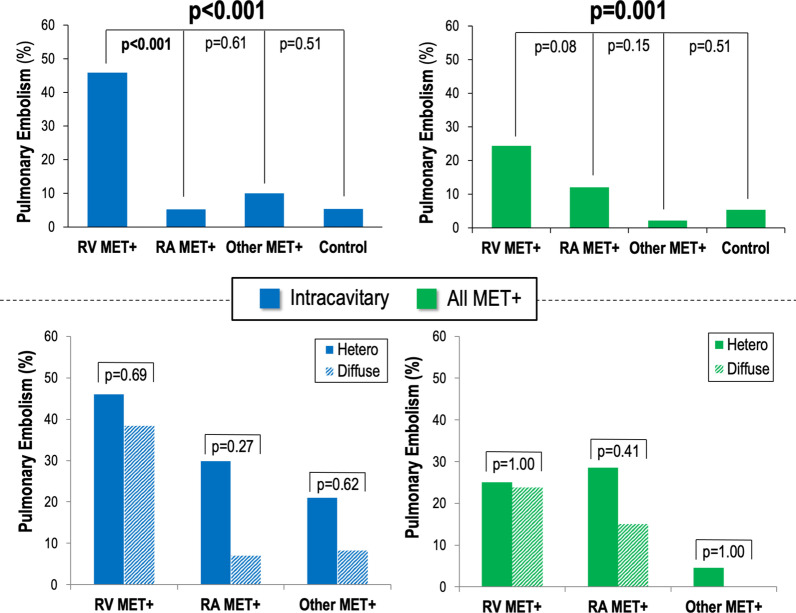
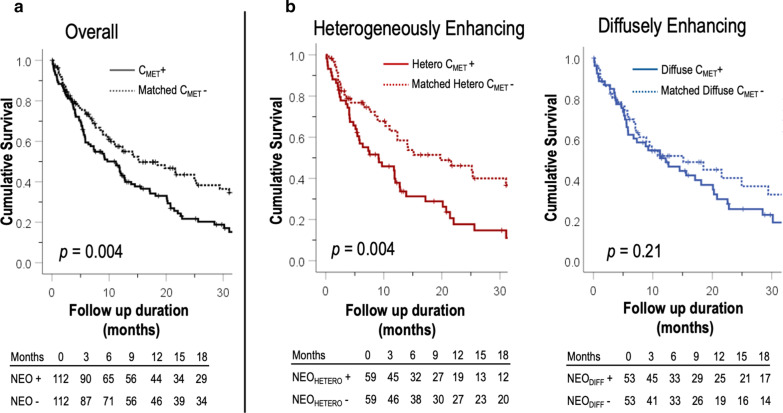
Results: 224 patients were studied, including 112 patients with CMET and unaffected (CMET -) controls matched for systemic cancer etiology/stage. CMET enhancement pattern varied (53% heterogeneous, 47% diffuse). Quantitative analyses were consistent with lesion classification; CNR was higher and SNR lower in heterogeneously enhancing CMET (p < 0.001)-paralleled by larger size based on linear dimensions (p < 0.05). Contrast-enhancement pattern did not vary based on lesion location (p = NS). Embolic events were similar between patients with diffuse and heterogeneous lesions (p = NS) but varied by location: Patients with right-sided lesions had threefold more pulmonary emboli (20% vs. 6%, p = 0.02); those with left-sided lesions had lower rates equivalent to controls (4% vs. 5%, p = 1.00). Mortality was higher among patients with CMET (hazard ratio [HR] = 1.64 [CI 1.17-2.29], p = 0.004) compared to controls, but varied by contrast-enhancement pattern: Diffusely enhancing CMET had equivalent mortality to controls (p = 0.21) whereas prognosis was worse with heterogeneous CMET (p = 0.005) and more strongly predicted by heterogeneous enhancement (HR = 1.97 [CI 1.23-3.15], p = 0.005) than lesion size (HR = 1.11 per 10 cm [CI 0.53-2.33], p = 0.79).
Conclusions: Contrast-enhancement pattern and location of CMET on CMR impacts prognosis. Embolic events vary by CMET location, with likelihood of PE greatest with right-sided lesions. Heterogeneous enhancement-a marker of tumor avascularity on LGE-CMR-is a novel marker of increased mortality risk.
Keywords: Cardiac neoplasm; Cardio-oncology; Cardiovascular magnetic resonance.
Conflict of interest statement
The authors disclose no relevant competing interests relevant to this research.
Figures
References
-
- National Cancer Institute: Surveillance, Epidemiology, and End Results Program. https://seer.cancer.gov/statistics/. 2019. Accessed 15 Jan 2020.
-
- Chan AT, Plodkowski AJ, Pun SC, et al. Prognostic utility of differential tissue characterization of cardiac neoplasm and thrombus via late gadolinium enhancement cardiovascular magnetic resonance among patients with advanced systemic cancer. J Cardiovasc Magn Reson. 2017;19:76. doi: 10.1186/s12968-017-0390-2. - DOI - PMC - PubMed
-
- Chan AT, Fox J, Perez Johnston R, et al. Late gadolinium enhancement cardiac magnetic resonance tissue characterization for cancer-associated cardiac masses: metabolic and prognostic manifestations in relation to whole-body positron emission tomography. J Am Heart Assoc. 2019;8:e011709. - PMC - PubMed
-
- Lam KY, Dickens P, Chan AC. Tumors of the heart. A 20-year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med. 1993;117:1027–1031. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
