

Sex- and Gender-Related Differences in Common Functional Gastroenterologic Disorders
- PMID: 33814075
- PMCID: PMC8075061
- DOI: 10.1016/j.mayocp.2020.10.004
Sex- and Gender-Related Differences in Common Functional Gastroenterologic Disorders
Abstract
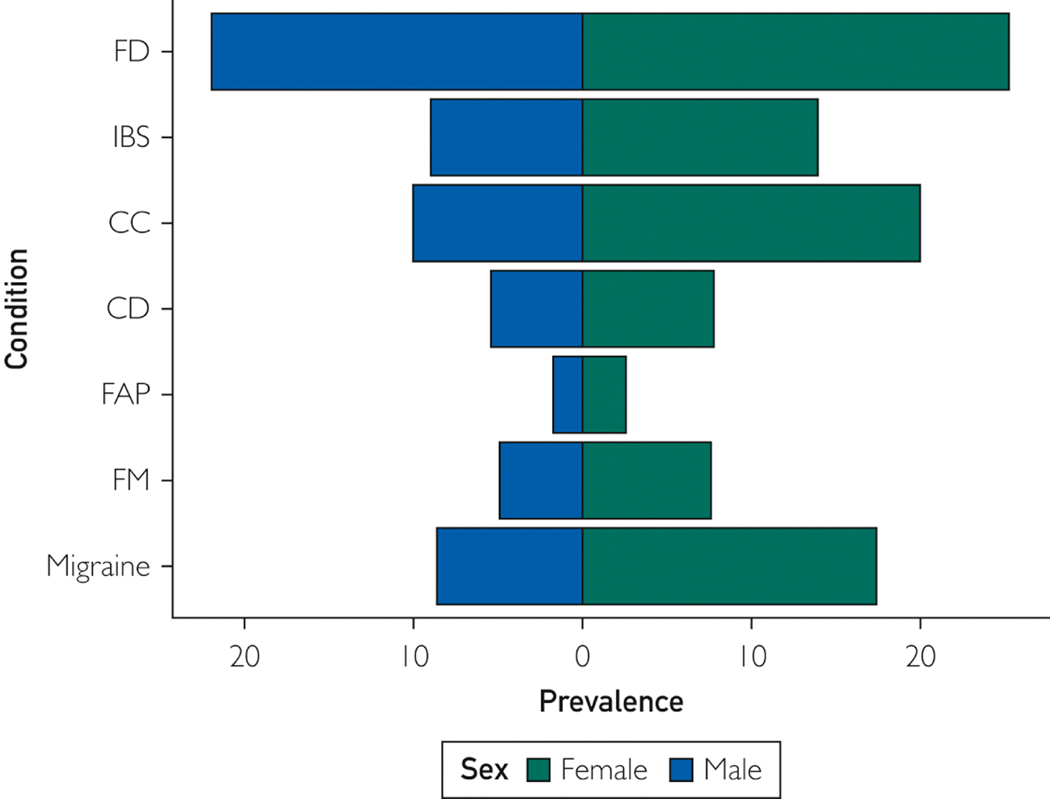
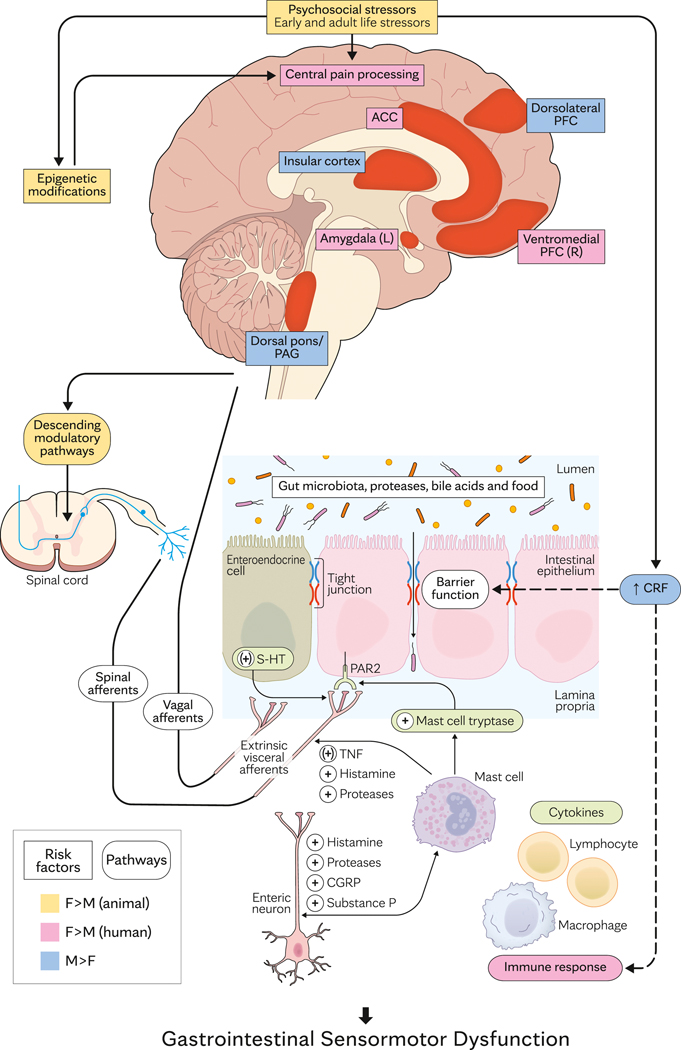
Functional gastrointestinal (GI) disorders (FGIDs) result from central and peripheral mechanisms, cause chronic remitting-relapsing symptoms, and are associated with comorbid conditions and impaired quality of life. This article reviews sex- and gender-based differences in the prevalence, pathophysiologic factors, clinical characteristics, and management of functional dyspepsia (FD) and irritable bowel syndrome (IBS) that together affect approximately 1 in 4 people in the United States. These conditions are more common in women. Among patients with IBS, women are more likely to have severe symptoms and coexistent anxiety or depression; constipation or bloating and diarrhea are more common in women and men, respectively, perhaps partly because defecatory disorders, which cause constipation, are more common in women. Current concepts suggest that biological disturbances (eg, persistent mucosal inflammation after acute gastroenteritis) interact with other environmental factors (eg, abuse) and psychological stressors, which influence the brain and gut to alter GI tract motility or sensation, thereby causing symptoms. By comparison to a considerable understanding of sex-based differences in the pathogenesis of visceral hypersensitivity in animal models, we know less about the contribution of these differences to FGID in humans. Slow gastric emptying and colon transit are more common in healthy women than in men, but effects of gonadal hormones on colon transit are less important than in rodents. Although increased visceral sensation partly explains symptoms, the effects of sex on visceral sensation, colonic permeability, and the gut microbiome are less prominent in humans than rodents. Whether sex or gender affects response to medications or behavioral therapy in FD or IBS is unclear because most patients in these studies are women.
Copyright © 2020 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Aziz I, Palsson OS, Tornblom H, Sperber AD, Whitehead WE, Simren M. The Prevalence and Impact of Overlapping Rome IV-Diagnosed Functional Gastrointestinal Disorders on Somatization, Quality of Life, and Healthcare Utilization: A Cross-Sectional General Population Study in Three Countries. American Journal of Gastroenterology. 2018;113:86–96. - PubMed
-
- Berkley KJ, Holdcroft A. Sex and Gender differences in pain. In: Wall PD, ed. Textbook of pain. 4 ed. Edinburgh: Churchill Livingstone; 2000:951–965.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
