

Role of chest radiography in the management of COVID-19 pneumonia: An overview and correlation with pathophysiologic changes
- PMID: 33814764
- PMCID: PMC7996675
- DOI: 10.4103/ijri.IJRI_967_20
Role of chest radiography in the management of COVID-19 pneumonia: An overview and correlation with pathophysiologic changes
Abstract
Background: Chest radiography (CXR) is a widely available baseline radiological modality in evaluating symptomatic patients with suspected or confirmed Covid-19 disease. Serial changes can help in monitoring the patients in conjunction with the clinical status of these patients in a hospital setting.
Purpose: The purpose of this study was to analyse the patterns of radiological findings on chest radiograph (CXR) for suspected and confirmed COVID-19 patients on initial presentation to the emergency medical services (EMS) on admission and to assess the progression and resolution.
Materials and methods: In this study, patients who presented to EMS of a multispeciality hospital as suspected or confirmed Covid-19 on consecutive reverse transcriptase polymerase chain reaction (RT-PCR). CXR was examined for findings of haziness, patterns and distribution of opacities. Progression and regression of findings in serial CXR were studied and evaluated with the clinical and laboratory parameters. High resolution CT (HRCT) chest was performed initially for some patients.
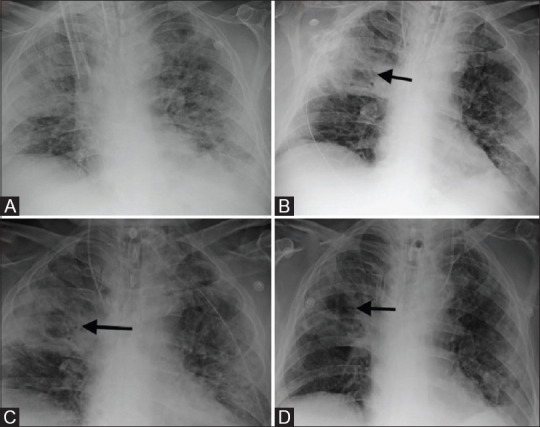
Results: 756 RT-PCR confirmed COVID-19 patients were included in our study who had initial CXR. 510 (67.46%) of our patients with positive initial RT-PCR showed abnormal baseline CXR. The abnormal findings were described as haziness akin to ground glass opacities (GGO) on CT, peripheral opacities, patchy parenchymal opacities and consolidation. Peripheral opacities and lower zone distribution were the commonest pattern of CXR abnormalities with bilateral involvement. The severity of findings on serial CXR and radiographic regression was studied along with follow-up to assess response to treatment. Forty-six patients showed features of acute lung injury (ALI). Complications and new CXR findings were reported for patients who were given ventilator support.
Conclusion: CXR is a valuable baseline radiological investigation on hospital admission in symptomatic patients with suspected or confirmed Covid-19 presenting to the EMS as it helps to monitor the progress and regression of the disease in conjunction with clinical findings.
Keywords: Acute lung injury; Covid-19 pneumonia; ventilator-associated pneumonia.
Copyright: © 2021 Indian Journal of Radiology and Imaging.
Conflict of interest statement
There are no conflicts of interest.
Figures




















References
-
- Cevik M, Kuppalli K, Kindrachuk J, Peiris M. Virology, transmission, and pathogenesis of SARS-CoV-2? BMJ. 2020;371:m3862. doi: 10.1136/bmj.m3862. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources