

Escalation and de-escalation of mechanical circulatory support in cardiogenic shock
- PMID: 33815013
- PMCID: PMC8005884
- DOI: 10.1093/eurheartj/suab007
Escalation and de-escalation of mechanical circulatory support in cardiogenic shock
Abstract
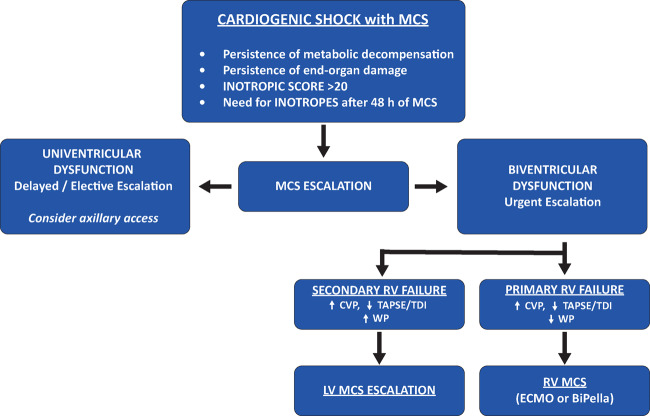
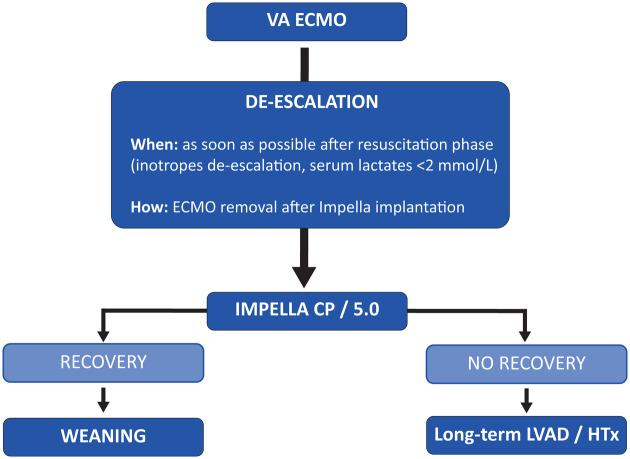
Cardiogenic shock (CS) is a clinical entity that includes a wide spectrum of different scenarios. Mechanical circulatory support (MCS) plays a fundamental role in the contemporary treatment of CS, and device selection is a key element in determining optimal treatment in this complex population. Cardiac support with mechanical devices should allow reduction and complete weaning from inotropes. Persistence of elevated left ventricular (LV) filling pressures, pulmonary congestion, metabolic decompensation, and end-organ damage during current MCS are criteria for MCS escalation. Precise diagnosis of the underlying cause of right ventricular (RV) failure is fundamental for undertaking the correct escalation strategy. In the setting of both MCS escalation and de-escalation, it is important to select a strategy in relation to long-term perspectives (bridge-to-recovery, bridge-to-LV assist device, or bridge-to-heart transplantation). Small retrospective studies have demonstrated that the BiPella approach is feasible, reduces cardiac filling pressures and improves cardiac output across a range of causes of CS. Simultaneous LV and RV device implantation and lower RV afterload may be associated with better outcomes in biventricular CS, but prospective studies are still required.
Keywords: Cardiogenic shock; Mechanical circulatory support; Unloading; Ventricular dysfunction.
Published on behalf of the European Society of Cardiology. © The Author(s) 2021.
Figures
Similar articles
-
Acute Biventricular Mechanical Circulatory Support for Cardiogenic Shock.J Am Heart Assoc. 2017 Oct 20;6(10):e006670. doi: 10.1161/JAHA.117.006670. J Am Heart Assoc. 2017. PMID: 29054842 Free PMC article.
-
Review of Pathophysiology of Cardiogenic Shock and Escalation of Mechanical Circulatory Support Devices.Curr Cardiol Rep. 2023 Apr;25(4):213-227. doi: 10.1007/s11886-023-01843-4. Epub 2023 Feb 27. Curr Cardiol Rep. 2023. PMID: 36847990 Review.
-
ECPELLA 2.0-Minimally invasive biventricular groin-free full mechanical circulatory support with Impella 5.0/5.5 pump and ProtekDuo cannula as a bridge-to-bridge concept: A first-in-man method description.J Card Surg. 2020 Jan;35(1):195-199. doi: 10.1111/jocs.14283. Epub 2019 Oct 14. J Card Surg. 2020. PMID: 31609509
-
Bridge to durable left ventricular assist device for refractory cardiogenic shock.J Thorac Cardiovasc Surg. 2017 Apr;153(4):752-762.e5. doi: 10.1016/j.jtcvs.2016.10.085. Epub 2016 Nov 16. J Thorac Cardiovasc Surg. 2017. PMID: 27988030
-
Advancements in mechanical circulatory support for patients in acute and chronic heart failure.J Thorac Dis. 2017 Oct;9(10):4070-4083. doi: 10.21037/jtd.2017.09.89. J Thorac Dis. 2017. PMID: 29268418 Free PMC article. Review.
Cited by
-
Role of acute mechanical circulatory support devices in cardiogenic shock.Indian J Thorac Cardiovasc Surg. 2023 Jul;39(Suppl 1):25-46. doi: 10.1007/s12055-023-01484-w. Epub 2023 Mar 28. Indian J Thorac Cardiovasc Surg. 2023. PMID: 37525710 Free PMC article. Review.
-
Management of Post-Myocardial Infarction Right Ventricular Failure.J Soc Cardiovasc Angiogr Interv. 2022 Nov 26;2(1):100526. doi: 10.1016/j.jscai.2022.100526. eCollection 2023 Jan-Feb. J Soc Cardiovasc Angiogr Interv. 2022. PMID: 39132546 Free PMC article. Review.
-
Differential utilization of Impella devices, extracorporeal membrane oxygenation, and combined therapies as escalation and de-escalation strategies.Eur Heart J Suppl. 2023 Dec 13;25(Suppl I):I32-I38. doi: 10.1093/eurheartjsupp/suad131. eCollection 2023 Dec. Eur Heart J Suppl. 2023. PMID: 38093771 Free PMC article.
-
Outcomes after heart transplantation in patients who have undergone a bridge-to-bridge strategy.JTCVS Open. 2022 Sep 8;12:255-268. doi: 10.1016/j.xjon.2022.08.011. eCollection 2022 Dec. JTCVS Open. 2022. PMID: 36590736 Free PMC article.
-
Monitoring MCS patients on the intensive care unit: integrating haemodynamic assessment, laboratory data, and imaging techniques for timely detection of deterioration and recovery.Eur Heart J Suppl. 2023 Dec 13;25(Suppl I):I24-I31. doi: 10.1093/eurheartjsupp/suad130. eCollection 2023 Dec. Eur Heart J Suppl. 2023. PMID: 38093766 Free PMC article.
References
-
- Basir MB, Schreiber TL, Grines CL, Dixon SR, Moses JW, Maini BS, Khandelwal AK, Ohman EM, O'Neill WW. Effect of early initiation of mechanical circulatory support on survival in cardiogenic shock. Am J Cardiol 2017;119:845–851. - PubMed
-
- Pieri M, Sorrentino T, Oppizzi M, Melisurgo G, Lembo R, Colombo A, Zangrillo A, Pappalardo F. The role of different mechanical circulatory support devices and their timing of implantation on myocardial damage and mid-term recovery in acute myocardial infarction related cardiogenic shock. J Interv Cardiol 2018;31:717–724. - PubMed
-
- Tongers J, Sieweke JT, Kühn C, Napp LC, Flierl U, Röntgen P, Schmitto JD, Sedding DG, Haverich A, Bauersachs J, Schäfer A. Early escalation of mechanical circulatory support stabilizes and potentially rescues patients in refractory cardiogenic shock. Circ Heart Fail 2020;13:e005853. - PubMed
-
- Tehrani BN, Truesdell AG, Sherwood MW, Desai S, Tran HA, Epps KC, Singh R, Psotka M, Shah P, Cooper LB, Rosner C, Raja A, Barnett SD, Saulino P, deFilippi CR, Gurbel PA, Murphy CE, O’Connor CM. Standardized team-based care for cardiogenic shock. J Am Coll Cardiol 2019;73:1659–1669. - PubMed
-
- Thiele H, Ohman EM, Desch S, Eitel I, de Waha S. Management of cardiogenic shock. Eur Heart J 2015;36:1223–1230. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources