

Aristolochic acid-associated urinary tract cancers: an updated meta-analysis of risk and oncologic outcomes after surgery and systematic review of molecular alterations observed in human studies
- PMID: 33815744
- PMCID: PMC7989132
- DOI: 10.1177/2042098621997727
Aristolochic acid-associated urinary tract cancers: an updated meta-analysis of risk and oncologic outcomes after surgery and systematic review of molecular alterations observed in human studies
Abstract
Background: The risk of primary aristolochic acid (AA)-associated urothelial carcinoma (AA-UC) has been summarized by a 2013-published meta-analysis. Given that additional evidence has been continuously reported by original studies, an updated meta-analysis is needed. Meanwhile, to complete the whole picture, a systematic review of molecular alterations observed in AA-urinary tract cancers (AA-UTC) was also performed.
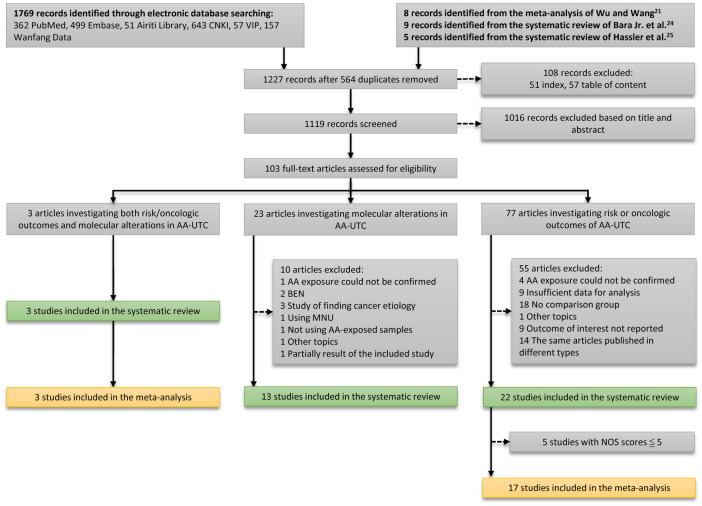
Methods: We searched PubMed, Embase and four Chinese databases up to October 2020. Observational studies comparing risk or oncologic outcomes of UTC between patients with and without AA exposure were eligible for systematic review and meta-analysis. Studies investigating molecular alterations in AA-UTC using human tissue samples were eligible for systematic review.
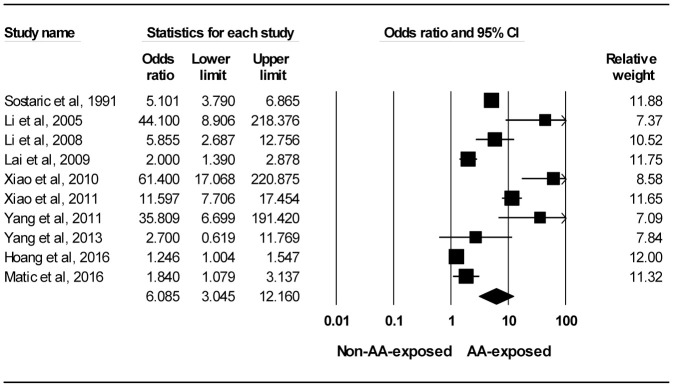
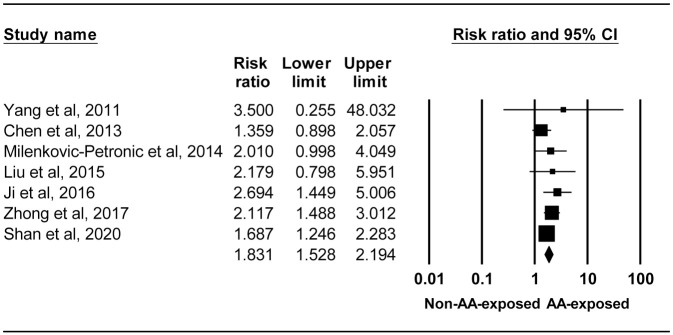
Results: In total, 38 and 20 studies were included in the systematic review and meta-analysis, respectively. Exposure to AA led to an overall increased risks of primary UTC [UC and renal cell carcinoma (RCC)] (OR 6.085, 95% CI 3.045-12.160) and postoperatively recurrent UC (RR 1.831, 95% CI 1.528-2.194). Subgroup analysis of postoperative primary AA-upper tract UC (AA-UTUC) showed increased risks of bladder recurrence (adjusted RR 1.949, 95% CI 1.462-2.597) and contralateral UTUC recurrence (crude RR 3.760, 95% CI 2.225-6.353), worse overall survival (adjusted HR 2.025, 95% CI 1.432-2.865) and worse disease-specific survival (adjusted HR 3.061, 95% CI 1.190-7.872), but no effect on cancer-specific survival (adjusted HR 0.772, 95% CI 0.269-2.215). High mutation load with AA mutational signature presenting largely in the putative driver genes was observed in AA-UTUC. In contrast, AA mutational signature is rarely found in the mutated RCC driver genes and the mutation load in AA-RCC is low. Therefore, AA has different roles in the genesis of UTUC and RCC.
Conclusions: Implementing effective strategies to completely protect people from exposure to AA is urgently needed. Additionally, more effort should be made in identifying the precise carcinogenic mechanisms of AA to determine the future treatment strategies.
Plain language summary: Risk, recurrence and survival outcomes after surgery and molecular changes possibly involved in the genesis of aristolochic acid-associated urinary tract cancers Background: The association between aristolochic acid (AA) and primary urothelial carcinoma (UC) has been summarized by a 2013-published meta-analysis. Given that additional evidence has been reported in the past 7 years, an updated meta-analysis is needed. Meanwhile, to complete the whole picture, a systematic review of molecular changes possibly involved in AA-mediated urinary tract carcinogenesis was also performed. Methods: We searched PubMed, Embase and four Chinese databases for human studies up to October 2020. Studies comparing the risk of urinary tract cancer (UTC) between patients with and without AA exposure and studies investigating the molecular changes in AA-associated UTC (AA-UTC) using human tissue samples were eligible for inclusion. Thirty-eight studies were finally included. Results: The results showed that exposure to AA was associated with a 6-fold increased risk of primary UTC (UC and renal cell carcinoma, RCC) and a 1.8-fold increased risk of postoperatively recurrent UC. After studies reporting primary AA-upper tract UC (AA-UTUC) were analyzed, a 1.9-fold increased risk of bladder recurrence and a 3.8-fold increased risk of contralateral UTUC recurrence was observed. Additionally, exposure to AA worsened the postoperative survival of patients with UTUC by a 2-fold increased risk of overall death and a 3-fold increased risk of death from other diseases and recurrences. However, there was no effect on death due to cancer. Lastly, AA seemed to play different roles in the etiology of UTUC and RCC based on the observations of different mutation loads and different distributions of AA-induced mutations in AA-UTUC and AA-RCC samples. Conclusions: Implementing effective strategies to completely protect people from exposure to AA is urgently needed. Moreover, more effort should be made in identifying the precise carcinogenic mechanisms of AA-UTC to determine the future treatment strategies.
Keywords: aristolochic acid; bladder recurrence; contralateral upper tract urothelial carcinoma recurrence; molecular alterations; oncologic outcomes; updated meta-analysis; updated systematic review; upper tract urothelial carcinoma; urothelial carcinoma.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: Yu-Chan Kang, Ming-Hong Chen, Chung-Ying Lin, Chih-Yun Lin and Yen-Ta Chen declare that they have no conflict of interest.
Figures
References
-
- Gökmen MR, Cosyns JP, Arlt VM, et al.. The epidemiology, diagnosis, and management of aristolochic acid nephropathy: a narrative review. Ann Intern Med 2013; 158: 469–477. - PubMed
-
- Lemy A, Wissing KM, Rorive S, et al.. Late onset of bladder urothelial carcinoma after kidney transplantation for end-stage aristolochic acid nephropathy: a case series with 15-year follow-up. Am J Kidney Dis 2008; 51: 471–477. - PubMed
-
- Jelaković B, Dika Ž, Arlt VM, et al.. Balkan endemic nephropathy and the causative role of aristolochic acid. Semin Nephrol 2019; 39: 284–296. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
