

A Simple Physical Therapy Algorithm Is Successful in Decreasing Skilled Nursing Facility Length of Stay and Increasing Cost Savings After Hip Fracture With No Increase in Adverse Events
- PMID: 33815865
- PMCID: PMC7995299
- DOI: 10.1177/2151459321998615
A Simple Physical Therapy Algorithm Is Successful in Decreasing Skilled Nursing Facility Length of Stay and Increasing Cost Savings After Hip Fracture With No Increase in Adverse Events
Abstract
Introduction: Shorter length of stays (LOS) at a Skilled Nursing Facility (SNF) after hip fracture surgery would be expected to lead to costs savings for the healthcare system. Evidence also suggests that shorter SNF stays also leads to improved 30-day outcomes, thus compounding this value proposition. Our Integrated Fragility Hip Fracture Program created a simple algorithm at discharge to provide each post-operative hip fracture patient with an expected SNF LOS. We studied whether this intervention produced a shorter SNF LOS and other observable short-term outcomes.
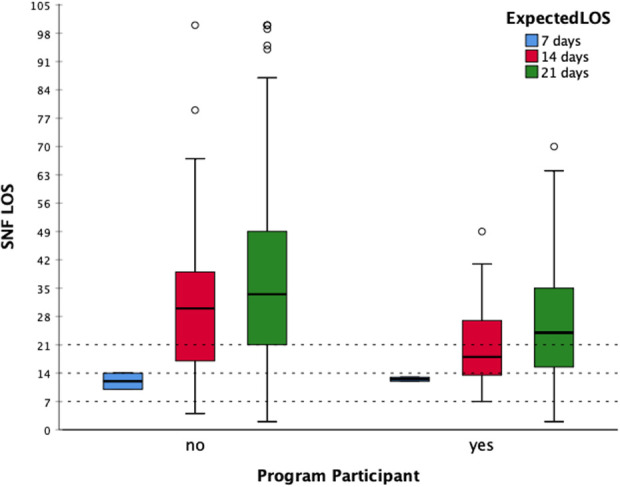
Methods: We retrospectively reviewed all original Medicare hip fracture patients treated with operative fixation who were admitted to our hospital in 2015, 2017 and 2018. We selected patients who were discharged to a single SNF following hospitalization, and excluded patients with incomplete records. The algorithm for the expected LOS recommendation was based on the degree of assistance the patient needed for ambulation: 7 days ("0-person assist"), 14 days ("1-person assist"), or 21 days ("2-person assist"). We compare the SNF LOS of our hip fracture patient population between those discharged to a program participant, those SNF that agreed to this algorithm, and those discharged to a non-program participant SNF.
Results: We identified 246 patients meeting our selection criteria. 69 were discharged to a program participant SNF. Patients discharged to a participant SNF had similar baseline demographics and ASA distributions to those discharged to a non-participant provider. There was a statistically significant difference in length of stay between the groups, with program participant patients spending an average of 23 days at the SNF while the control group spent an average of 31 days. (p < 0.001). Program participant discharges were also associated with additional cost savings. There was no significant difference in ED visits within 90 days of discharge.
Discussion: SNF LOS for geriatric hip fractures can be decreased with implementation of a simple physical therapy driven algorithm based on the patient's ambulatory independence at hospital discharge. Conclusion: This is a simple, yet completely unique program that seems to have increased the value of healthcare provided.
Keywords: economics of medicine; fragility fractures; geriatric nursing; physical medicine and rehabilitation; trauma surgery.
© The Author(s) 2021.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Comparing post-acute rehabilitation use, length of stay, and outcomes experienced by Medicare fee-for-service and Medicare Advantage beneficiaries with hip fracture in the United States: A secondary analysis of administrative data.PLoS Med. 2018 Jun 26;15(6):e1002592. doi: 10.1371/journal.pmed.1002592. eCollection 2018 Jun. PLoS Med. 2018. PMID: 29944655 Free PMC article.
-
What happens to patients when they fracture their hip during a skilled nursing facility stay?J Am Med Dir Assoc. 2015 Sep 1;16(9):767-74. doi: 10.1016/j.jamda.2015.03.026. Epub 2015 May 2. J Am Med Dir Assoc. 2015. PMID: 25944177 Free PMC article.
-
Effect of Obesity on Postacute Outcomes of Skilled Nursing Facility Residents with Hip Fracture.J Am Geriatr Soc. 2018 Jul;66(6):1108-1114. doi: 10.1111/jgs.15334. Epub 2018 Apr 3. J Am Geriatr Soc. 2018. PMID: 29616500 Free PMC article.
-
Comparison of discharge functional status after rehabilitation in skilled nursing, home health, and medical rehabilitation settings for patients after hip fracture repair.Arch Phys Med Rehabil. 2014 Feb;95(2):209-17. doi: 10.1016/j.apmr.2013.05.031. Epub 2013 Jul 10. Arch Phys Med Rehabil. 2014. PMID: 23850612
-
Family Partnerships, Palliative Care and End of Life.2018 Apr 12. In: Hertz K, Santy-Tomlinson J, editors. Fragility Fracture Nursing: Holistic Care and Management of the Orthogeriatric Patient [Internet]. Cham (CH): Springer; 2018. Chapter 11. 2018 Apr 12. In: Hertz K, Santy-Tomlinson J, editors. Fragility Fracture Nursing: Holistic Care and Management of the Orthogeriatric Patient [Internet]. Cham (CH): Springer; 2018. Chapter 11. PMID: 31314468 Free Books & Documents. Review.
Cited by
-
Hospital Variation in Skilled Nursing Facility Use After Coronary Artery Bypass Graft Surgery.J Am Heart Assoc. 2024 Jan 16;13(2):e029833. doi: 10.1161/JAHA.123.029833. Epub 2024 Jan 9. J Am Heart Assoc. 2024. PMID: 38193303 Free PMC article.
-
Rehabilitation of Frail Older Adults after Hip Fracture Surgery: Predictors for the Length of Geriatric Rehabilitation Stay at a Skilled Nursing Home.J Clin Med. 2024 Aug 3;13(15):4547. doi: 10.3390/jcm13154547. J Clin Med. 2024. PMID: 39124813 Free PMC article.
-
Boosting inpatient exercise after hip fracture using an alternative workforce: a mixed methods implementation evaluation.BMC Geriatr. 2024 Feb 14;24(1):149. doi: 10.1186/s12877-024-04730-x. BMC Geriatr. 2024. PMID: 38350882 Free PMC article.
References
-
- Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12): 1726–1733. - PubMed
-
- Braithwaite RS, Col NF, Wong JB. Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc. 2003;51(3):364–370. - PubMed
-
- Magaziner J, Fredman L, Hawkes W, et al. Changes in functional status attributable to hip fracture: a comparison of hip fracture patients to community-dwelling aged. Am J Epidemiol. 2003;157(11):1023–1031. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
