

Computed Tomography Features of Gastric Cancer Patients With DNA Mismatch Repair Deficiency
- PMID: 33816249
- PMCID: PMC8012908
- DOI: 10.3389/fonc.2021.619439
Computed Tomography Features of Gastric Cancer Patients With DNA Mismatch Repair Deficiency
Abstract
Objective: To explore the computed tomography (CT) features of gastric cancer (GC) patients with DNA mismatch repair deficiency (dMMR).
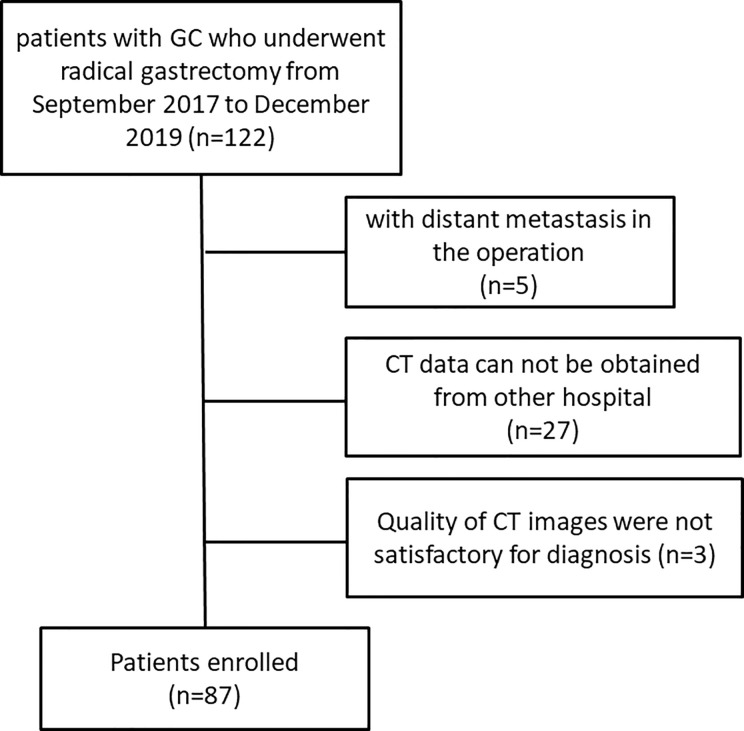
Materials and methods: This study reviewed the clinical and CT features of GC patients with dMMR, confirmed by the postoperative results, between September 2017 and December 2019. The expression pattern of MMR major proteins (MLH1, MSH2, MSH6, and PMS2) in immunohistochemistry was used to confirm the MMR status in GC tissues. The correlation between pre-treatment CT features and MMR status was statistically analyzed.
Results: A total of 28 patients with GC were diagnosed as dMMR in our study, and 49 patients were MMR-proficient (pMMR). The tumor locations were significantly different between the dMMR and pMMR groups (p = 0.006). The CT tumor thickness, CT long and short diameters of the largest lymph node, and the number of lymph nodes on CT of the dMMR group were significantly different from the pMMR group.
Conclusion: The dMMR GC exhibited a lower stomach location, smaller tumor thickness and lymph node diameter, and fewer lymph nodes on CT imaging.
Keywords: computed tomography; gastric cancer; microsatellite instability; mismatch repair deficiency; prognosis.
Copyright © 2021 Cao, Lai, Xu, Lu, Chen, Zhang and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Association of status of mismatch repair protein expression and EB virus infection with clinicopathological parameters in 886 gastric adenocarcinoma patients].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 May 25;24(5):440-448. doi: 10.3760/cma.j.issn.441530-20200910-00518. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 34000774 Chinese.
-
[Difference analysis of somatic mutations between deficient mismatch repair and proficient mismatch repair gene related with colorectal cancer].Zhonghua Zhong Liu Za Zhi. 2021 Oct 23;43(10):1088-1093. doi: 10.3760/cma.j.cn112152-20190719-00448. Zhonghua Zhong Liu Za Zhi. 2021. PMID: 34695900 Chinese.
-
Clinicopathological features and prognostic value of mismatch repair protein deficiency in gastric cancer.Int J Clin Exp Pathol. 2018 May 1;11(5):2579-2587. eCollection 2018. Int J Clin Exp Pathol. 2018. PMID: 31938371 Free PMC article.
-
ESMO recommendations on microsatellite instability testing for immunotherapy in cancer, and its relationship with PD-1/PD-L1 expression and tumour mutational burden: a systematic review-based approach.Ann Oncol. 2019 Aug 1;30(8):1232-1243. doi: 10.1093/annonc/mdz116. Ann Oncol. 2019. PMID: 31056702
-
Microsatellite instability testing and its role in the management of colorectal cancer.Curr Treat Options Oncol. 2015 Jul;16(7):30. doi: 10.1007/s11864-015-0348-2. Curr Treat Options Oncol. 2015. PMID: 26031544 Free PMC article. Review.
Cited by
-
The Clinicopathological Characteristics and Prognoses of dMMR Gastric Adenocarcinoma Patients.Gastroenterol Res Pract. 2021 Dec 9;2021:4269781. doi: 10.1155/2021/4269781. eCollection 2021. Gastroenterol Res Pract. 2021. PMID: 34925504 Free PMC article.
-
A radiomics signature derived from CT imaging to predict MSI status and immunotherapy outcomes in gastric cancer: a multi-cohort study.BMC Cancer. 2024 Apr 1;24(1):404. doi: 10.1186/s12885-024-12174-0. BMC Cancer. 2024. PMID: 38561648 Free PMC article.
-
CT-based radiomic nomogram for preoperative prediction of DNA mismatch repair deficiency in gastric cancer.Front Oncol. 2022 Sep 16;12:883109. doi: 10.3389/fonc.2022.883109. eCollection 2022. Front Oncol. 2022. PMID: 36185292 Free PMC article.
-
Nomogram based on dual-energy CT-derived extracellular volume fraction for the prediction of microsatellite instability status in gastric cancer.Front Oncol. 2024 May 24;14:1370031. doi: 10.3389/fonc.2024.1370031. eCollection 2024. Front Oncol. 2024. PMID: 38854729 Free PMC article.
-
A noninvasive nomogram model based on CT features to predict DNA mismatch repair deficiency in gastric cancer.Front Oncol. 2023 Mar 9;13:1066352. doi: 10.3389/fonc.2023.1066352. eCollection 2023. Front Oncol. 2023. PMID: 36969034 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous