

Deficits in Monocyte Function in Age Related Macular Degeneration: A Novel Systemic Change Associated With the Disease
- PMID: 33816525
- PMCID: PMC8010137
- DOI: 10.3389/fmed.2021.634177
Deficits in Monocyte Function in Age Related Macular Degeneration: A Novel Systemic Change Associated With the Disease
Abstract
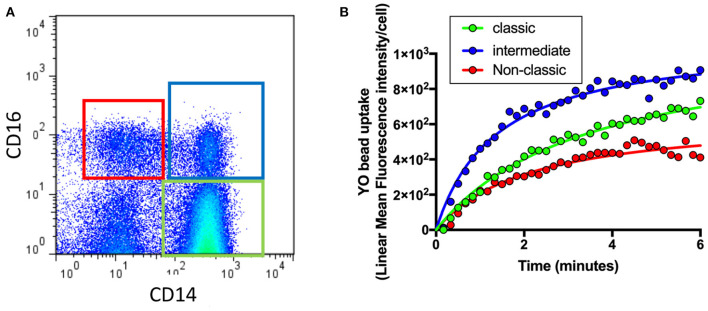
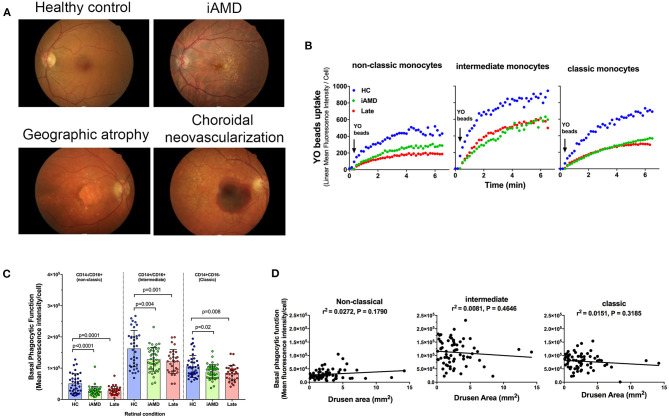
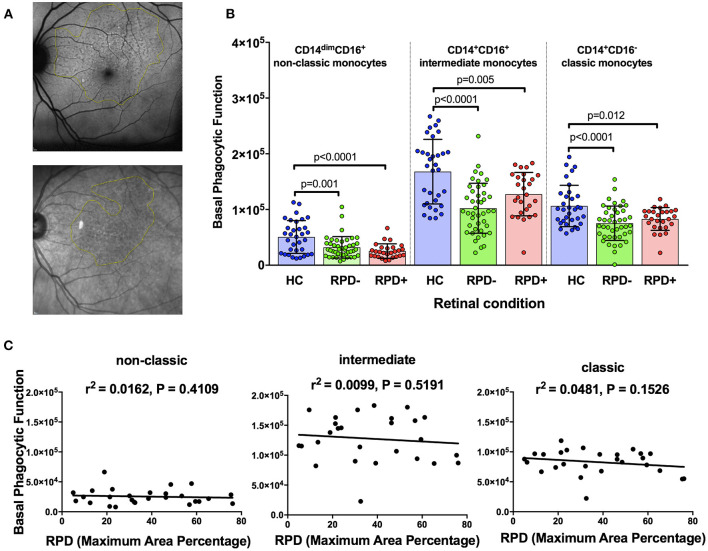
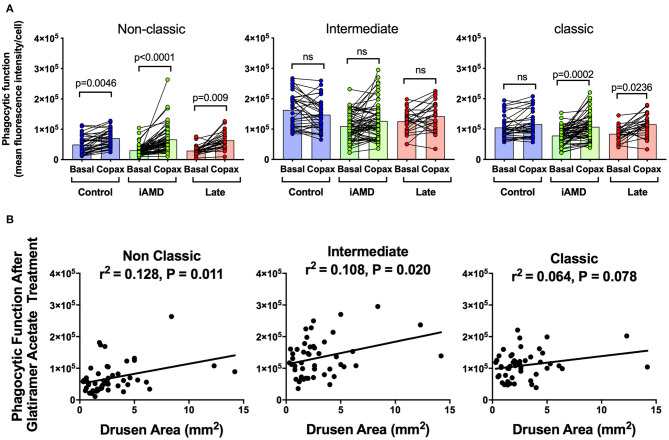
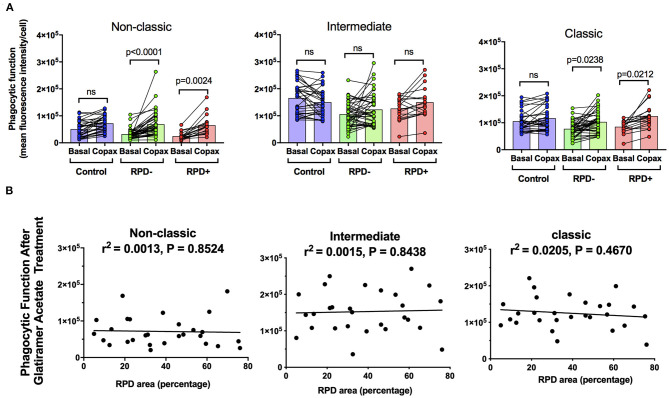
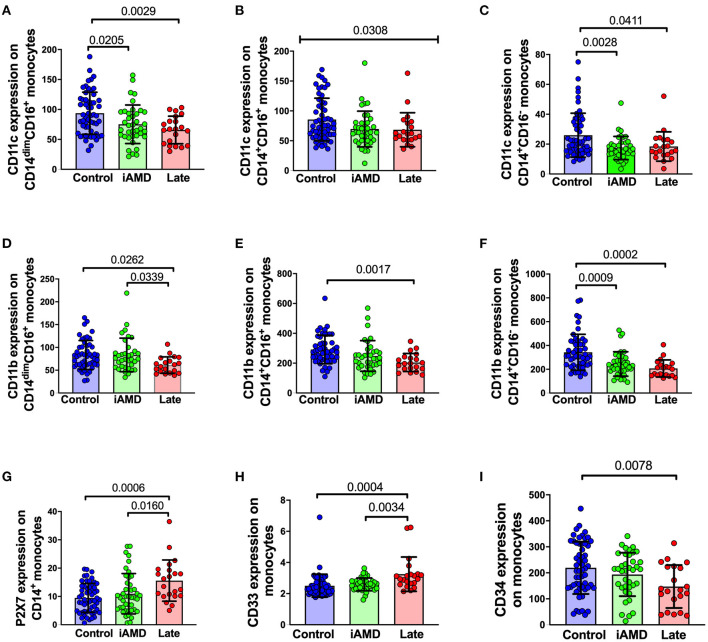
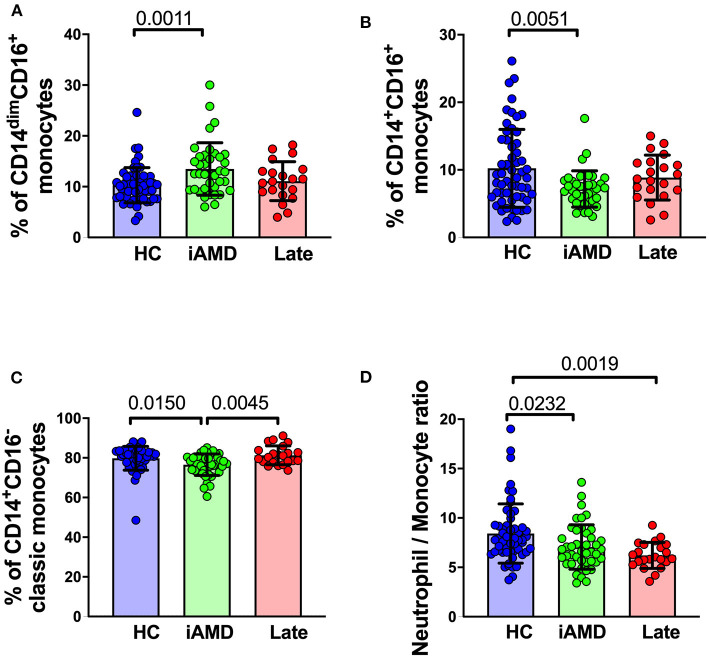
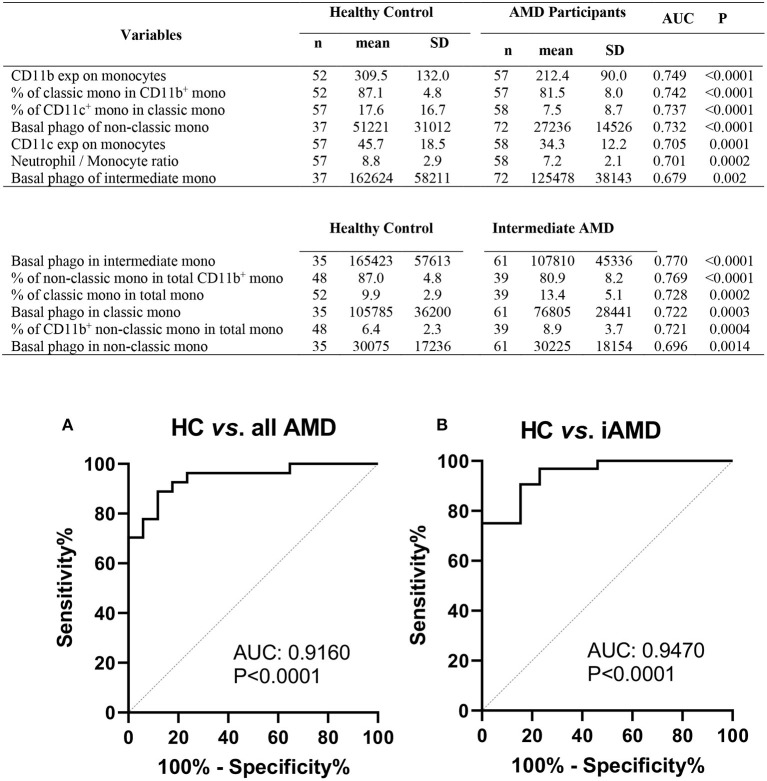
Age-related macular degeneration (AMD) is characterized by the accumulation of debris in the posterior eye. In this study we evaluated peripheral blood monocyte phagocytic function at various stages of AMD and in aged matched control participants. Real-time tri-color flow cytometry was used to quantify phagocytic function of peripheral blood monocyte subsets (non-classic, intermediate and classic) isolated from subjects with intermediate or late AMD and compared with age matched healthy controls. Assessment of phagocytic function of monocytes isolated from those with and without reticular pseudodrusen was also made, and the effect of glatiramer acetate on phagocytic function assessed. Phagocytic function was reduced in all subjects with AMD, irrespective of stage of disease. However, there was no correlation between phagocytic function and drusen load, nor any difference between the level of phagocytosis in those with or without reticular pseudodrusen. Treatment with glatiramer acetate increased phagocytosis of classical and non-classical monocytes, normalizing the reduction in phagocytosis observed in those with AMD. These findings suggest that defective systemic phagocytosis is associated with both intermediate and late stages of AMD, highlighting a potential role in the accumulation of debris that occurs early in the disease process. Assessing peripheral monocyte phagocytic function provides further insights into the etiology of this disease and offer a novel therapeutic target.
Keywords: drusen; glatiramer acetate; monocytes; phagocytosis; reticular pseudodrusen.
Copyright © 2021 Gu, Huang, Avula, Caruso, Drysdale, Vessey, Ou, Fowler, Liu, Lin, Horton, Masters, Wiley, Guymer and Fletcher.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources