

Efficacy of Prehabilitation Including Exercise on Postoperative Outcomes Following Abdominal Cancer Surgery: A Systematic Review and Meta-Analysis
- PMID: 33816546
- PMCID: PMC8017317
- DOI: 10.3389/fsurg.2021.628848
Efficacy of Prehabilitation Including Exercise on Postoperative Outcomes Following Abdominal Cancer Surgery: A Systematic Review and Meta-Analysis
Abstract
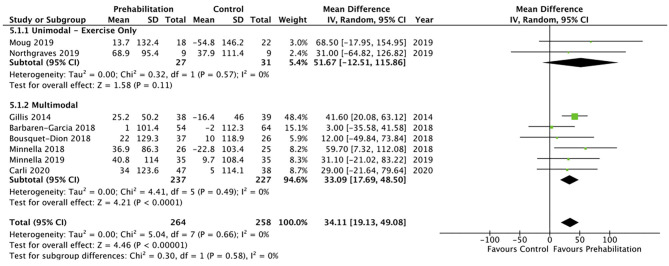
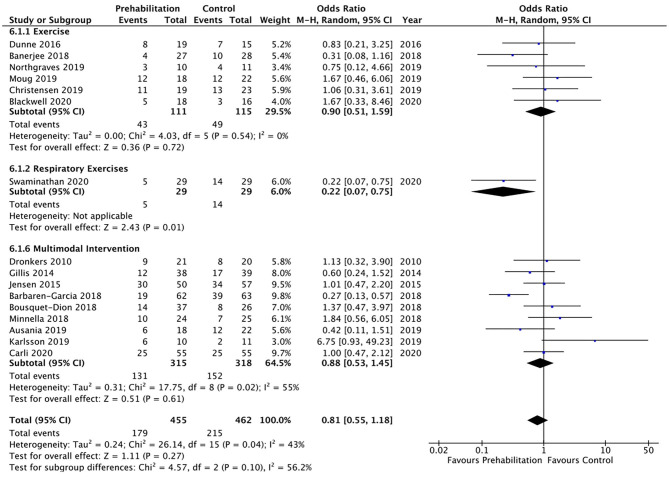
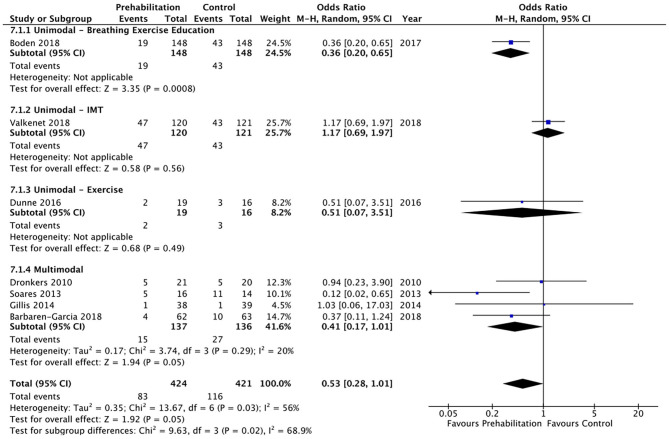
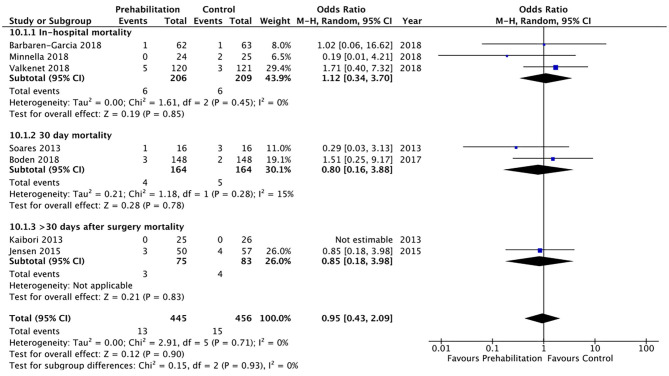
Objectives: This systematic review set out to identify, evaluate and synthesise the evidence examining the effect of prehabilitation including exercise on postoperative outcomes following abdominal cancer surgery. Methods: Five electronic databases (MEDLINE 1946-2020, EMBASE 1947-2020, CINAHL 1937-2020, PEDro 1999-2020, and Cochrane Central Registry of Controlled Trials 1991-2020) were systematically searched (until August 2020) for randomised controlled trials (RCTs) that investigated the effects of prehabilitation interventions in patients undergoing abdominal cancer surgery. This review included any form of prehabilitation either unimodal or multimodal that included whole body and/or respiratory exercises as a stand-alone intervention or in addition to other prehabilitation interventions (such as nutrition and psychology) compared to standard care. Results: Twenty-two studies were included in the systematic review and 21 studies in the meta-analysis. There was moderate quality of evidence that multimodal prehabilitation improves pre-operative functional capacity as measured by 6 min walk distance (Mean difference [MD] 33.09 metres, 95% CI 17.69-48.50; p = <0.01) but improvement in cardiorespiratory fitness such as preoperative oxygen consumption at peak exercise (VO2 peak; MD 1.74 mL/kg/min, 95% CI -0.03-3.50; p = 0.05) and anaerobic threshold (AT; MD 1.21 mL/kg/min, 95% CI -0.34-2.76; p = 0.13) were not significant. A reduction in hospital length of stay (MD 3.68 days, 95% CI 0.92-6.44; p = 0.009) was observed but no effect was observed for postoperative complications (Odds Ratio [OR] 0.81, 95% CI 0.55-1.18; p = 0.27), pulmonary complications (OR 0.53, 95% CI 0.28-1.01; p = 0.05), hospital re-admission (OR 1.07, 95% CI 0.61-1.90; p = 0.81) or postoperative mortality (OR 0.95, 95% CI 0.43-2.09, p = 0.90). Conclusion: Multimodal prehabilitation improves preoperative functional capacity with reduction in hospital length of stay. This supports the need for ongoing research on innovative cost-effective prehabilitation approaches, research within large multicentre studies to verify this effect and to explore implementation strategies within clinical practise.
Keywords: cancer; meta-analysis; prehabilitation; surgery; systematic review.
Copyright © 2021 Waterland, McCourt, Edbrooke, Granger, Ismail, Riedel and Denehy.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
-
- Ismail H, Cormie P, Burbury K, Waterland J, Denehy L, Riedel B. Prehabilitation prior to major cancer surgery: training forsurgery to optimize physiologic reserve to reduce postoperativecomplications. Curr Anesthesiol Rep. (2018) 8:375–85. 10.1007/s40140-018-0300-7 - DOI
-
- Macmillian Cancer Support . Prehabilitation for People With Cancer: Principles and Guidance for Prehabilitation Within the Management and Support of People With Cancer. (2019). Available online at: www.macmillian.org.uk/assets/prehabilitation-guideline-for-people-with-c... (accessed July 01, 2020).
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical