

Targeting treatment options for castration-resistant prostate cancer
- PMID: 33816699
- PMCID: PMC8012826
Targeting treatment options for castration-resistant prostate cancer
Abstract
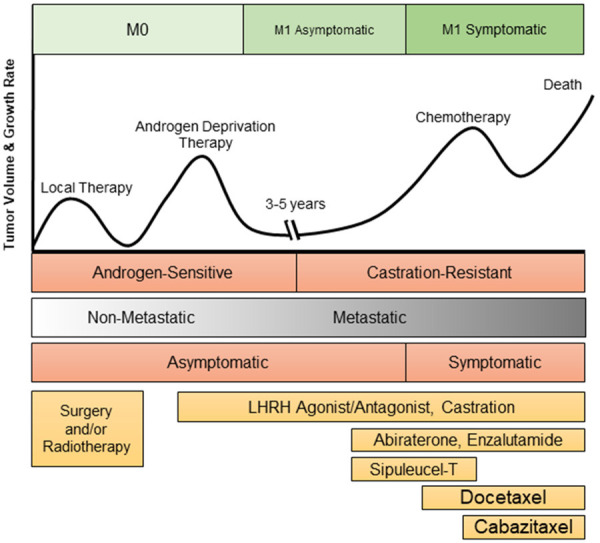
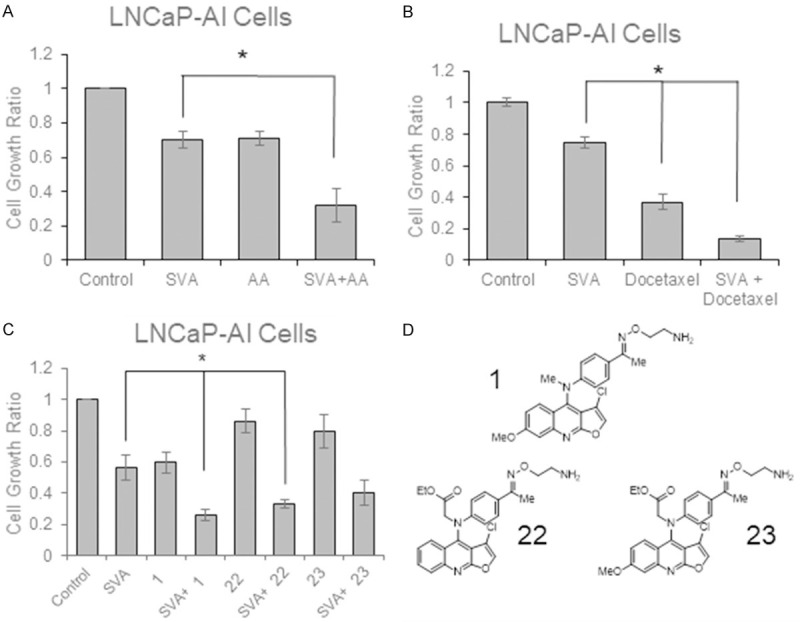
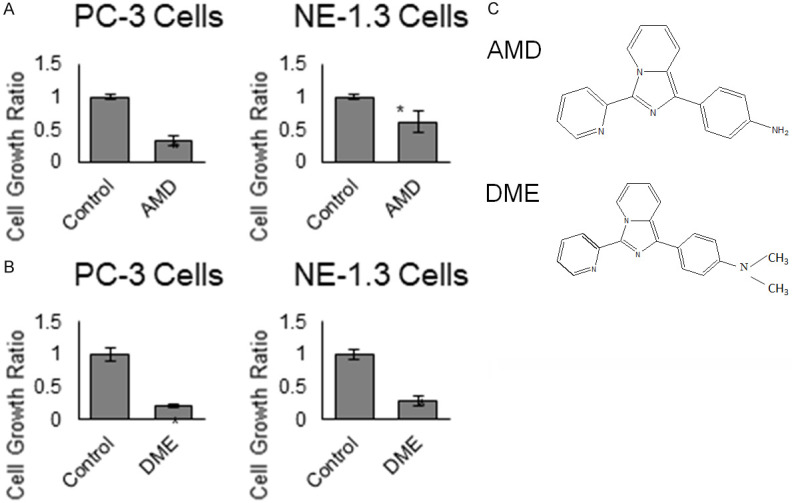
Prostate cancer (PCa) is the most commonly diagnosed solid tumor and the second leading cause of cancer-related deaths in U.S. men in 2020. Androgen-deprivation therapy (ADT) is the standard of care for metastatic PCa. Unfortunately, PCa relapse often occurs one to two years after initiation of ADT, resulting in the development of castration-resistant PCa (CRPCa), a lethal disease. While several anticancer agents such as docetaxel, abiraterone acetate, and enzalutamide are currently utilized to extend a patient's life after development of CRPCa, patients will eventually succumb to the disease. Hence, while targeting androgen signaling and utilization of docetaxel remain the most crucial agents for many of these combinations, many studies are attempting to exploit other vulnerabilities of PCa cells, such as inhibition of key survival proteins, anti-angiogenesis agents, and immunotherapies. This review will focus on discussing recent advances on targeting therapy. Several novel small molecules will also be discussed.
Keywords: Prostate cancer; androgen deprivation therapy; castration-resistant prostate cancer; combination treatment; targeting therapy.
AJCEU Copyright © 2021.
Conflict of interest statement
None.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30. - PubMed
-
- Mohler JL, Armstrong AJ, Bahnson RR, D’Amico AV, Davis BJ, Eastham JA, Enke CA, Farrington TA, Higano CS, Horwitz EM, Hurwitz M, Kane CJ, Kawachi MH, Kuettel M, Lee RJ, Meeks JJ, Penson DF, Plimack ER, Pow-Sang JM, Raben D, Richey S, Roach M 3rd, Rosenfeld S, Schaeffer E, Skolarus TA, Small EJ, Sonpavde G, Srinivas S, Strope SA, Tward J, Shead DA, Freedman-Cass DA. Prostate cancer, version 1.2016. J Natl Compr Canc Netw. 2016;14:19–30. - PubMed
-
- Liu J, Geller J, Albert J, Kirshner M. Acute effects of testicular and adrenal cortical blockade on protein synthesis and dihydrotestosterone content of human prostate tissue. J Clin Endocrinol Metab. 1985;61:129–133. - PubMed
-
- Taplin ME, Bubley GJ, Shuster TD, Frantz ME, Spooner AE, Ogata GK, Keer HN, Balk SP. Mutation of the androgen-receptor gene in metastatic androgen-independent prostate cancer. N Engl J Med. 1995;332:1393–1398. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources