

Clinical usefulness of Edinburgh CT criteria in patients with lobar intracerebral hemorrhage
- PMID: 33817333
- PMCID: PMC7995326
- DOI: 10.1177/2396987320975736
Clinical usefulness of Edinburgh CT criteria in patients with lobar intracerebral hemorrhage
Abstract
Background: Identifying the cause of intracerebral hemorrhage (ICH) is relevant to optimize its management. We aimed to assess the applicability and utility of the Edinburgh CT criteria for cerebral amyloid angiopathy (CAA) in an unselected cohort of hospitalized patients.
Patients and methods: We retrospectively applied the Edinburgh criteria to the first available brain CTs of patients hospitalized for a first-ever lobar ICH in the district of L'Aquila from 2011 to 2017. ICH characteristics and outcomes were compared according to the presence of the Edinburgh CT criteria, including associated subarachnoid hemorrhage (aSAH) and finger-like projections (FLPs). The outcome of ICH in-hospital mortality was assessed with multivariate logistic regression analysis. We adopted the Edinburgh criteria, age, NIHSS and Glasgow Coma Scale scores, systolic blood pressure, antiplatelet treatment, ICH volume, and intraventricular extension on admission as covariates.
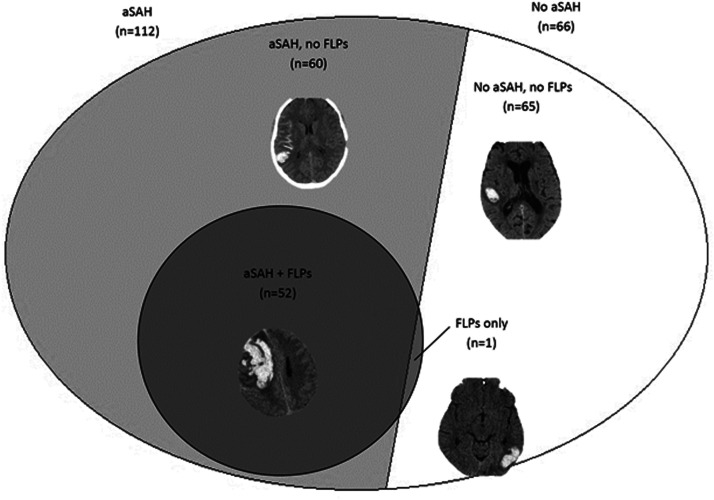
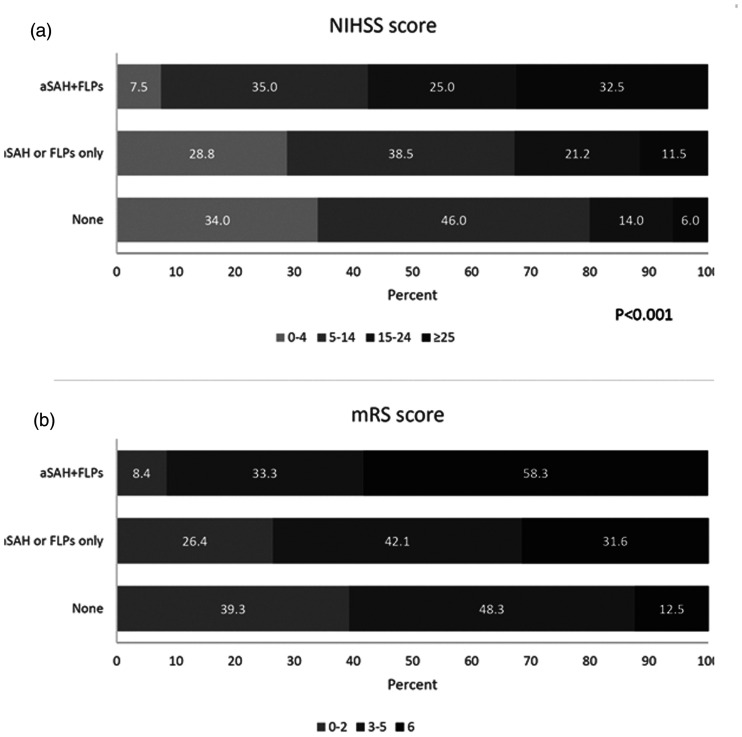
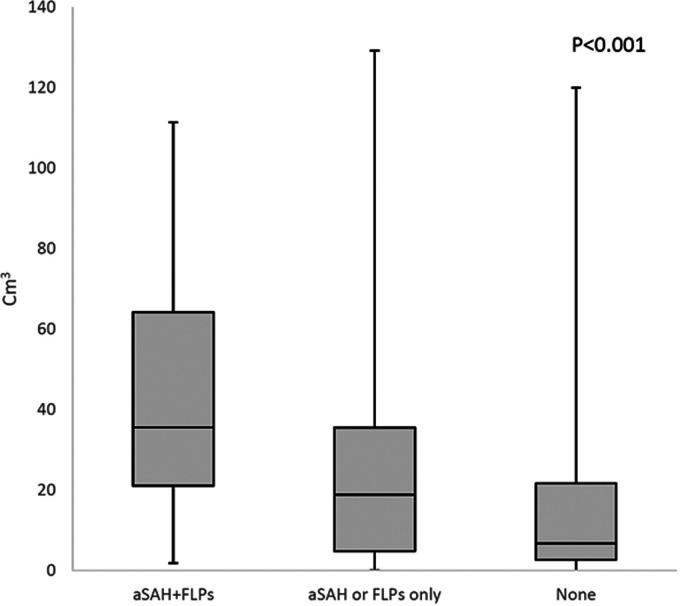
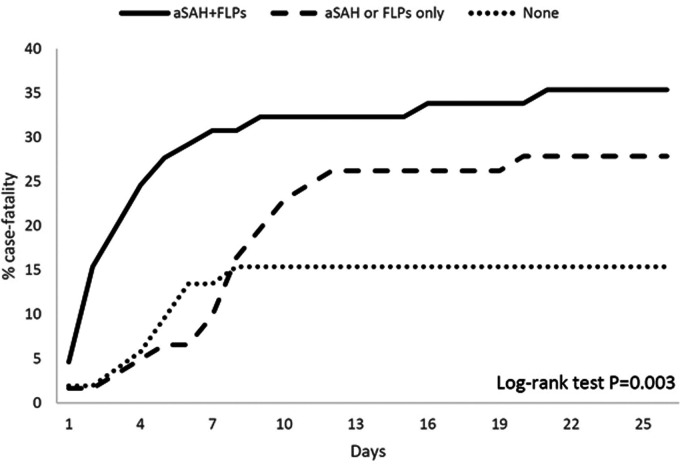
Results: Of 178 patients with lobar ICH, 52 (29.2%) had aSAH+FLPs, 60 (33.7%) aSAH only, 1 (0.6%) FLPs, and 65 (36.5%) none. Patients with aSAH+FLPs were older (79.0 ± 9.2 years) than those with only one criterion or none (74.0 ± 15.3 and 72.2 ± 13.8 years, respectively; P = 0.020). Patients with aSAH+FLPs also had more severe ICH at onset, higher in-hospital case-fatality (log rank test P = 0.003) and higher mRS scores at discharge (P < 0.001) as compared to those fulfilling one or none of the Edinburgh criteria. Low Glasgow Coma Scale score was the only factor independently associated to in-hospital case-fatality (odds ratio per point increase 0.51; 95% confidence interval, 0.32-0.91; P = 0.021).
Discussion: Our data suggest the applicability of the Edinburgh CT criteria in a hospital setting. The presence of those criteria reflects ICH clinical severity.
Conclusions: Applying the Edinburgh CT criteria might help refining the diagnosis and improving the management of patients with lobar ICH.
Keywords: Intracerebral hemorrhage; amyloid angiopathy; computed tomography; imaging; prognosis; stroke.
© European Stroke Organisation 2020.
Conflict of interest statement
Declaration of conflicting interests: RThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: O reports non-financial relationships with Novartis, Allergan, and Teva outside the submitted work; SS reports Dr Sacco reports personal fees and non-financial support from Allergan, personal fees and nonfinancial support from Abbott, personal fees and non-financial support from Eli Lilly, personal fees and non-financial support from Novartis, personal fees and non-financial support from TEVA, personal fees from Medscape, other from Bayer, other from Pfizer, other from Medtronic, other from Starmed, other from Bristol-Myers Squibb, and other from Daiichi-Sankyo outside the submitted work; all the other Authors declare no conflicts of interest.
Figures
References
-
- Feigin VL, Lawes CM, Bennett DA, et al.. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol 2009; 8: 355–369. - PubMed
-
- Sacco S, Marini C, Toni D, et al.. Incidence and 10-year survival of intracerebral hemorrhage in a population-based registry. Stroke 2009; 40: 394–399. - PubMed
-
- Sacco S, Ornello R, Degan D, et al.. Declining incidence of intracerebral hemorrhage over two decades in a population-based study. Eur J Neurol 2016; 23: 1627–1634. - PubMed
-
- van Asch CJ, Luitse MJ, Rinkel GJ, et al.. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and Meta-analysis. Lancet Neurol 2010; 9: 167–176. - PubMed
-
- Qureshi AI, Tuhrim S, Broderick JP, et al.. Spontaneous intracerebral hemorrhage. N Engl J Med 2001; 344: 1450–1460. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
