

Assessment of pulmonary arterial circulation 3 months after hospitalization for SARS-CoV-2 pneumonia: Dual-energy CT (DECT) angiographic study in 55 patients
- PMID: 33817609
- PMCID: PMC8008988
- DOI: 10.1016/j.eclinm.2021.100778
Assessment of pulmonary arterial circulation 3 months after hospitalization for SARS-CoV-2 pneumonia: Dual-energy CT (DECT) angiographic study in 55 patients
Abstract
Background: During COVID-19, the main manifestations of the disease are not only pneumonia but also coagulation disorders. The purpose of this study was to evaluate pulmonary vascular abnormalities 3 months after hospitalization for SARS-CoV-2 pneumonia in patients with persistent respiratory symptoms.
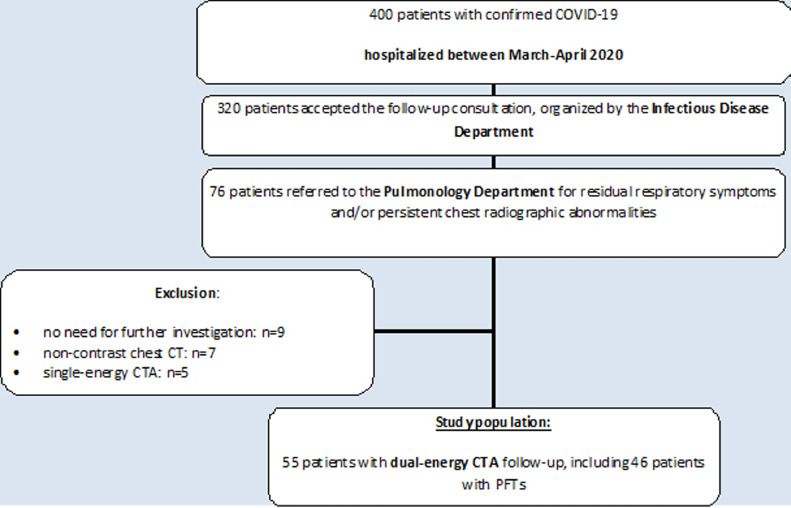
Methods: Among the 320 patients who participated in a systematic follow-up 3 months after hospitalization, 76 patients had residual symptoms justifying a specialized follow-up in the department of pulmonology. Among them, dual-energy CT angiography (DECTA) was obtained in 55 patients.
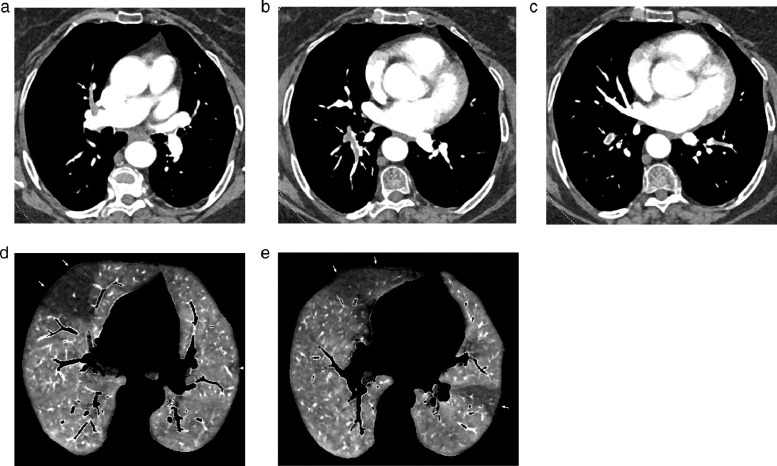
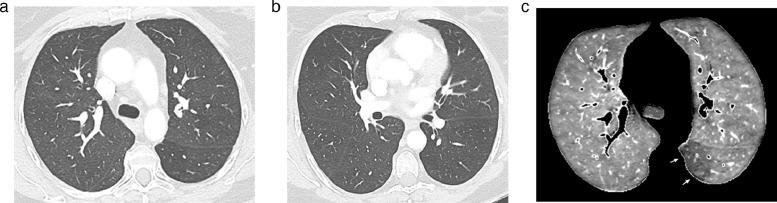
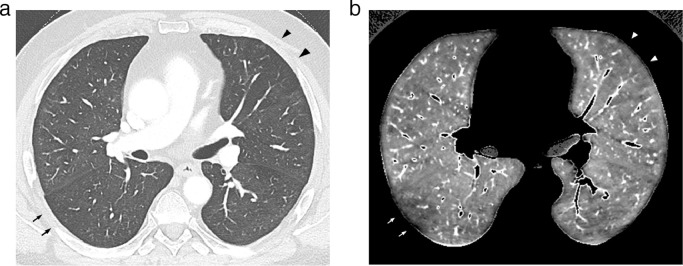
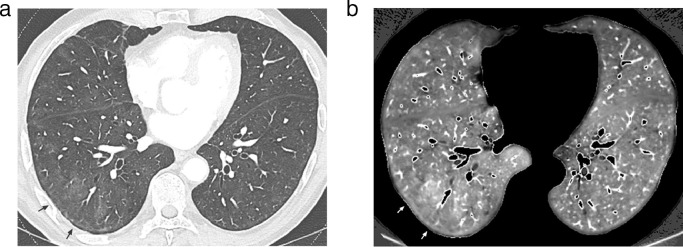
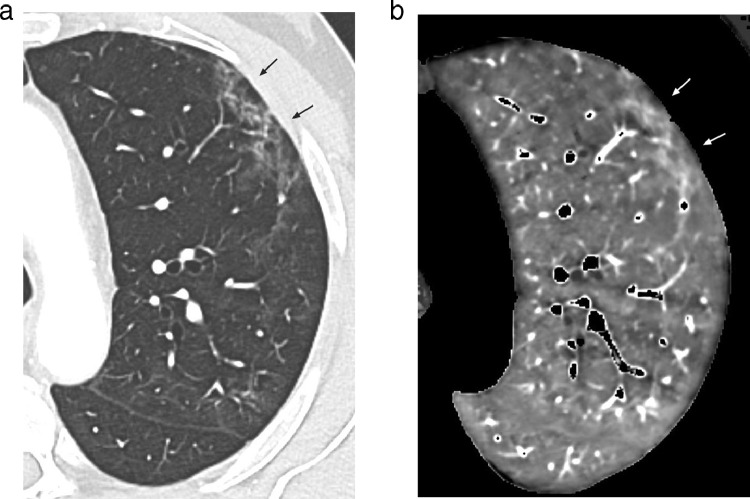
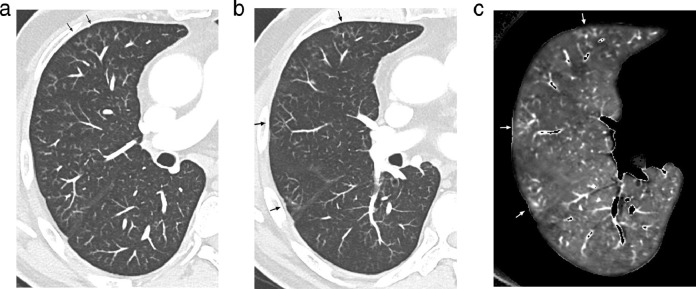
Findings: The 55 patients had partial (n = 40; 72.7%) or complete (n = 15; 27.3%) resolution of COVID-19 lung infiltration. DECTA was normal in 52 patients (52/55; 94.6%) and showed endoluminal filling defects in 3 patients (3/55; 5.4%) at the level of one (n = 1) and two (n = 1) segmental arteries of a single lobe and within central and peripheral arteries (n = 1). DECT lung perfusion was rated as non-interpretable (n = 2;3.6%), normal (n = 17; 30.9%) and abnormal (n = 36; 65.5%), the latter group comprising 32 patients with residual COVID-19 opacities (32/36; 89%) and 4 patients with normal lung parenchyma (4/36; 11%). Perfusion abnormalities consisted of (a) patchy defects (30/36; 83%), (b) PE-type defects (6/36; 16.6%) with (n = 1) or without proximal thrombosis (n = 5); and (c) focal areas of hypoperfusion (2/36; 5.5%). Increased perfusion was seen in 15 patients, always matching GGOs, bands and/or vascular tree-in- bud patterns.
Interpretation: DECT depicted proximal arterial thrombosis in 5.4% of patients and perfusion abnormalities suggestive of widespread microangiopathy in 65.5% of patients. Lung microcirculation was abnormal in 4 patients with normal lung parenchyma.
Keywords: COVID-19; CT angiography; Dual-energy CT; Lung perfusion; Pulmonary embolism.
© 2021 Published by Elsevier Ltd.
Conflict of interest statement
Author MRJ received nonfinancial support for clinical research purposes from Siemens Healthineers. Author JR received personal fees as consultant for Siemens Healthineers and non-financial support for clinical research purposes. All other authors have nothing to declare.
Figures
References
-
- Raptis C.A., Hammer M.M., Short R.G. Chest CT and coronavirus disease (COVID-19): a critical review of the literature to date. AJR. 2020;215:1–4. - PubMed
-
- Han H., Yang L., Liu R. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin Chem Lab Med. 2020;58:1116–1120. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
