

Does giving birth in a "birth environment room" versus a standard birth room lower augmentation of labor? - Results from a randomized controlled trial
- PMID: 33817626
- PMCID: PMC8010388
- DOI: 10.1016/j.eurox.2021.100125
Does giving birth in a "birth environment room" versus a standard birth room lower augmentation of labor? - Results from a randomized controlled trial
Abstract
Objective: In the last decade, there has been an increased interest in exploring the impact of the physical birth environment on midwifery practice and women's birth experiences. This study is based on the hypothesis that the environment for birth needs greater attention to improve some of the existing challenges in modern obstetric practice, for example the increasing use of augmentation and number of interventions during delivery.
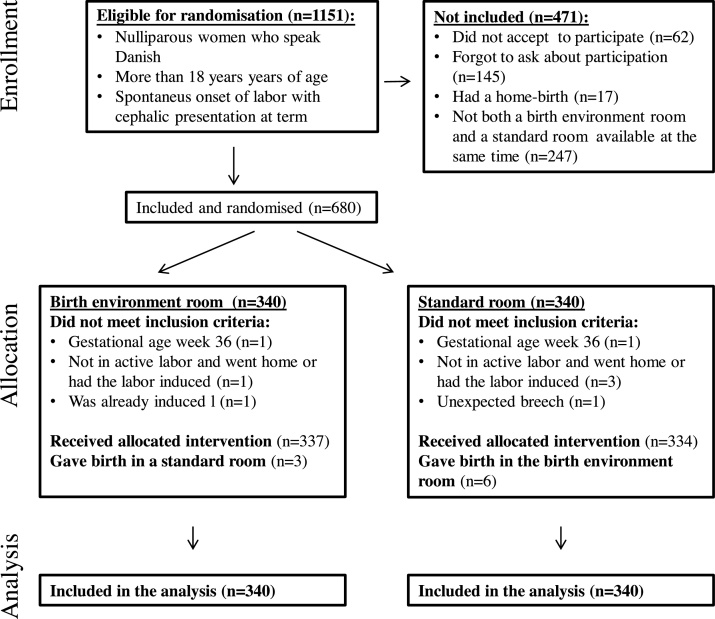
Study design: A randomized controlled trial was carried out to study the effect of giving birth in a specially designed "birth environment room" on the use of augmentation during labor. The study took place at the Department of Obstetrics and Gynecology, Herning Hospital, Denmark and included 680 nulliparous women in spontaneous labor at term with a fetus in cephalic presentation. Women were randomly allocated to either the "birth environment room" or a standard birth room. The primary outcome was augmentation of labor by use of oxytocin. Secondary outcomes were duration of labor, use of pharmacological pain relief, and mode of birth. Differences were estimated as relative risks (RR) and presented with 95% confidence intervals.
Results: No difference was found on the primary outcome, augmentation of labor (29.1% in the "birth environment room" versus 30.6% in the standard room, RR 0.97; 0.89-1.08). More women in the "birth environment room" used the bathtub (60.6% versus 52.4%, RR 1.18; 1.02-1.37), whereas a tendency to lower use of epidural analgesia (22.6% versus 28.2%) did not reach statistical significance (RR 0.87; 0.74-1.02). The chance of an uncomplicated birth was almost similar in the two groups (70.6% in the "birth environment room" versus 72.6% in the standard room, RR 0.97; 0.88-1.07) as were duration of labor (mean 7.9 hours in both groups).
Conclusions: Birthing in a specially designed physical birth environment did not lower use of oxytocin for augmentation of labor. Neither did it have any effect on duration of labor, use of pharmacological pain relief, and chance of birthing without complications. We recommend that future trials are conducted in birth units with greater improvement potentials.
Keywords: Birth environment; Birth experience; Birth outcome; Birth room design; Birth unit design; Oxytocin.
© 2021 Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




Similar articles
-
Study protocol for a randomised trial evaluating the effect of a "birth environment room" versus a standard labour room on birth outcomes and the birth experience.Contemp Clin Trials Commun. 2019 Feb 15;14:100336. doi: 10.1016/j.conctc.2019.100336. eCollection 2019 Jun. Contemp Clin Trials Commun. 2019. PMID: 30886935 Free PMC article.
-
The effect on the birth experience of women and partners of giving birth in a "birth environment room": A secondary analysis of a randomised controlled trial.Midwifery. 2022 Sep;112:103424. doi: 10.1016/j.midw.2022.103424. Epub 2022 Jul 7. Midwifery. 2022. PMID: 35850078 Clinical Trial.
-
Room4Birth - the effect of an adaptable birthing room on labour and birth outcomes for nulliparous women at term with spontaneous labour start: study protocol for a randomised controlled superiority trial in Sweden.Trials. 2019 Nov 19;20(1):629. doi: 10.1186/s13063-019-3765-x. Trials. 2019. PMID: 31744523 Free PMC article.
-
The effect of early oxytocin augmentation in labor: a meta-analysis.Obstet Gynecol. 2009 Sep;114(3):641-649. doi: 10.1097/AOG.0b013e3181b11cb8. Obstet Gynecol. 2009. PMID: 19701046 Review.
-
Delayed versus immediate pushing in the second stage of labor in women with neuraxial analgesia: a systematic review and meta-analysis of randomized controlled trials.Am J Obstet Gynecol. 2020 Aug;223(2):189-203. doi: 10.1016/j.ajog.2020.02.002. Epub 2020 Feb 15. Am J Obstet Gynecol. 2020. PMID: 32067972
Cited by
-
Impact of Birthing Room Design on Maternal Childbirth Experience: Results From the Room4Birth Randomized Trial.HERD. 2023 Jan;16(1):200-218. doi: 10.1177/19375867221124232. Epub 2022 Oct 14. HERD. 2023. PMID: 36239523 Free PMC article. Clinical Trial.
-
Implementing a new birthing room design: a qualitative study with a care provider perspective.BMC Health Serv Res. 2023 Oct 19;23(1):1122. doi: 10.1186/s12913-023-10051-3. BMC Health Serv Res. 2023. PMID: 37858103 Free PMC article. Clinical Trial.
References
-
- Tracy S.K., Sullivan E., Wang Y.A., Black D., Tracy M. Birth outcomes associated with interventions in labour amongst low risk women: a population-based study. Women Birth. 2007;20(2):41–48. - PubMed
-
- Patterson J.A., Roberts C.L., Ford J.B., Morris J.M. Trends and outcomes of induction of labour among nullipara at term. Aust New Zealand J Obstet Gynaecol. 2011;51(6):510–517. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
